PEDIATRIC ACETABULAR FRACTURES
JEFFREY J. METER, M.D., Resident, Orthopaedic Surgery
RICHARD KRUSE, D.O., Attending, Pediatric Orthopaedic Surgery
November 25, 1995
CLINICAL CASE PRESENTATION
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
History:
The patient is a 16 year old female that was previously in good health
when she was involved in a roll-over motor vehicle accident as an unrestrained
passenger, ejected from the vehicle. She landed in a field. She was taken
by ambulance to a nearby hospital and later transferred to the A.I. duPont
Institute for definitive treatment of a right acetabulum fracture, right
pelvic fracture, and non-displaced left clavicle fracture. After evaluation
with General Surgery for this multiple trauma victim, the patient's medical
problems were isolated to the right hip and pelvis. She was hemodynamically
stable with a benign abdomen. Although the pelvis grossly appeared stable,
motion of the hip caused significant pain. The limb was intact neurologically
and had strong pulses.
Radiographs:
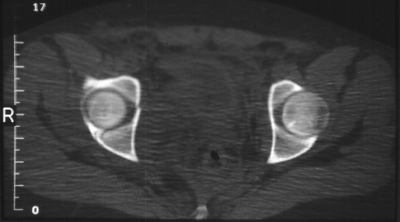
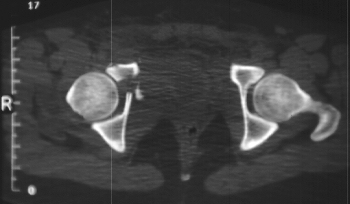
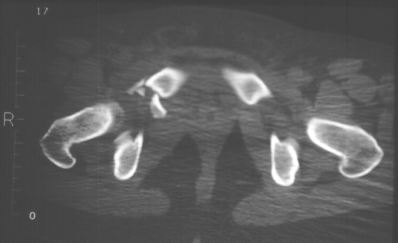
Radiographs revealed a vertical buckle fracture of the right inferior
sacrum, oblique fractures of the superior and inferior rami on the right
and a fracture through the medial acetabulum.  Obturator and iliac oblique
Obturator and iliac oblique  inlet and outlet pelvic views, and a thin cut CT
inlet and outlet pelvic views, and a thin cut CT
 with
3-D reconstruction of the acetabulum were performed.
with
3-D reconstruction of the acetabulum were performed. 

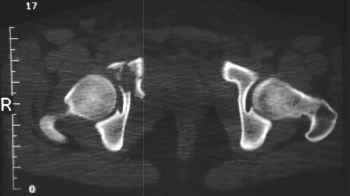
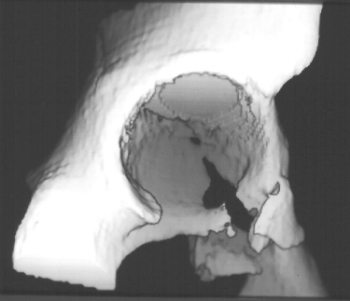
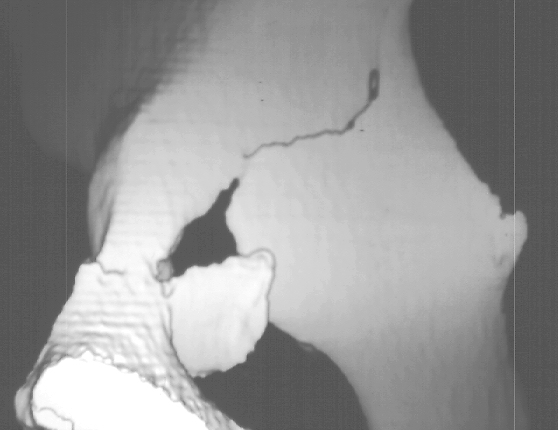
 These elucidated a comminuted anterior wall with fracture line extending
to the posterior column. The posterior column was non-displaced. The pelvic
fracture was non-displaced.
These elucidated a comminuted anterior wall with fracture line extending
to the posterior column. The posterior column was non-displaced. The pelvic
fracture was non-displaced.
Assessment:
- Right T-shaped acetabular fracture with anterior wall comminution.
- Right pelvic fracture, lateral compression, displaced ;5 mm.
Treatment:
Bed rest for five days, with progressive ambulation, toe-touch, on crutches.
FRACTURES OF THE ACETABULUM IN CHILDREN
Anatomy / Epidemiology
The acetabulum is cup-shaped, with the base of the cup flat and composed
of the triradiate cartilage (ilium, ischium, and pubis). Three secondary
centers around the acetabulum can be of importance. The os acetabuli forms
the anterior wall, the acetabular epiphysis forms the superior wall, and
the ischial epiphysis is inferiomedial. The volume of cartilage in the
child's acetabulum allows a greater capacity for energy absorption than
in adults. Thus, in children, fractures of the acetabulum are consistently
the result of high-energy trauma. In addition the cartilage can make the
diagnosis of fracture more difficult and can result in growth disturbance
about the acetabulum.
The incidence of acetabular fractures is not knowN. Recent studies at
Level I trauma centers have shown an admission rate for pelvic and acetabular
fractures of .5 - 7.5 %.
Classification
There is no classification of children's acetabular fractures, so we
must use Letournel and Judet and Salter-Harris. Letournel and Judet
A. Posterior wall fracture. B. Posterior column fracture. C. Anterior
wall fracture. D. Anterior column fracture. E. Transverse fracture. F.
Posterior column and posterior wall fracture. G. Transverse and posterior
wall fracture. H. T-shaped fracture. I. Anterior column and posterior hemitransverse
fracture. J. Both column fracture.
Management
INITIAL: Because of the strong association of pediatric acetabular fractures
with high-energy trauma, these patients should be transferred initially
to a trauma center. Management should initially be directed at a full primary
and secondary ATLS survey, to include large bore IV access and search for
related injuries: intra-abdominal, GU, intrathoracic, intracranial fractures
of the femur, skull, ribs, tibia, clavicle, facial bones, humerus
RADIOGRAPHIC: cervical, chest , AP pelvis, 45 degree oblique view of
Judet - obturator and iliac oblique to assess anterior column and posterior
columns, respectively
COMPUTED TOMOGRAPHY: R/O intra-articular loose fragments, Plan for surgery.
HIP ARTHROGRAM in young children in which hip fracture/dislocation suspected
Roof arc measurements
(Matta, et al.) Measurement of intact cartilage medially, anteromedially,
and posteromedially to vertex of acetabulum. Medial roof arc - A P, Anterior
roof arc - obturator oblique, Posterior roof arc - iliac oblique, If the
medial roof arc is less than 30 degrees, subluxation occurs
ACETABULAR FRACTURE SPECIFICALLY
Non-operative
Heeg, et al. Non-displaced or 1 mm: Bed rest, non-weight bearing ambulation
(monitored). Reducible with traction to 2 mm: skeletal traction (distal
femur)
Matta, et al. {(1 or 2) and 3}
- The presence of apparent congruence in both column fractures
- The presence of an adequate dome by roof arc measurements . -anterior
roof arc greater than or equal to 30 degrees, -medial roof arc greater
than or equal to 40 degrees, -posterior roof arc greater than or equal
to 50 degrees .
- The femoral head must remain congruous with the roof of the acetabulum
with the patient out of traction
OPEN REDUCTION, INTERNAL FIXATION
Indications
Involves weight-bearing surface, 2 mm displaced or an unstable posterior
wall fracture/dislocation
Approaches
Posterior wall: Kocher-Langenbeck Anterior column: ilioinguinal Transverse
and combined: extended iliofemoral or combined approach
Fixation
Most fractures need just lag screws may use 3.5 or 2.7 recon plates
Complications
Early: DVT, neurovascular injury, associated injuries. Late: premature
closure of the triradiate cartilate which leads to a small deep acetabulum
joint degeneration, femoral subluxation, AVN
Expected Results
Heeg, et : 23 acetabular fractures in children, age 2-17 years, F/U
8 years, 21 good or excellent results. Conservative gave good results when
minimal displacement, stable posterior fracture/dislocation, and Salter-Harris
I and II injuries.
Comminuted fractures and Salter-Harris 5 injuries gave worse results
- operated or not
Unstable posterior fracture-dislocations and central fracture-dislocations
need surgery
REFERENCES:
- Bond, S.I.; Gotschall, C.S.; Eichelberger, M.R. Predictors of abdominal
injury in children with pelvic fracture. J Trauma 31:1169-1173, 1991.
- Letournel, E.; Judet, R. Fractures of the Acetabulum. Berlin, Springer
Verlag, 1981.
- Matta, J.M.; Mehne, E.K.; Roff, R. Fractures of the acetabulum: Early
results of a prospective study. Clin Orthop 205:241-250, 1986.
- Matta, J.; Anderson, L.; Epstein, H.; and Henricks, P. Fractures of
the acetabulum. A retrospective analysis. Orthop. Trans. 6(3), 1982.
- Ponsetti, I.V. Growth and development of the acetabulum in the normal
child. J Bone Joint Surg 60-A:575-585, 1978.
- Quinby, W.C., Jr. Fractures of the pelvis and associated injuiries
in children. J Pediatr Surg 1:353-364,1966.
- Reed, M.H. Pelvic fractures in children. J Can Assoc Radiol 27:255-261,
1976.
- Swiontkowski, M.F. Fractures and dislocations about the hip and pelvis.
In: Swiontkowski, M.F. and Green, N.E. Skeletal Trauma in Children. Philadelphia,
W.B. Saunders, 1994, pp.307-343.
 Obturator and iliac oblique
Obturator and iliac oblique  inlet and outlet pelvic views, and a thin cut CT
inlet and outlet pelvic views, and a thin cut CT
 with
3-D reconstruction of the acetabulum were performed.
with
3-D reconstruction of the acetabulum were performed. 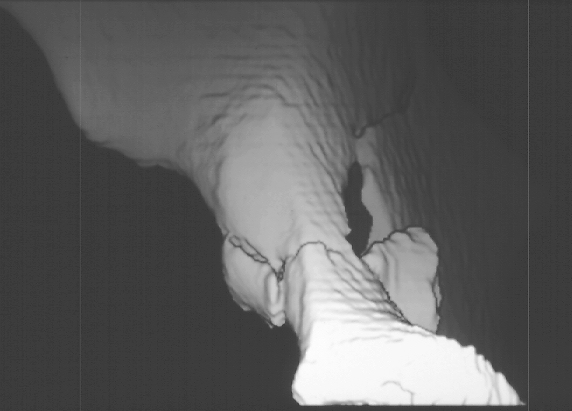
 These elucidated a comminuted anterior wall with fracture line extending
to the posterior column. The posterior column was non-displaced. The pelvic
fracture was non-displaced.
These elucidated a comminuted anterior wall with fracture line extending
to the posterior column. The posterior column was non-displaced. The pelvic
fracture was non-displaced.