IDIOPATHIC CHONDROLYSIS
FRANK CUCE, D.O., Orthopaedic Surgery Resident
KIRK W. DABNEY, M.D., Attending Pediatric Orthopaedic Surgeon
February 13, 1996
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY
This is a 12 year old Asian female with insidious onset of left hip
pain 4 months in duration. At one point, her pain was so severe she could
not bear weight and had to be picked up from school. She denies trauma
to the hip. She could not participate in sports secondary to pain and also
developed a limp with apparent leg length discrepancy secondary to pelvic
obliquity and local muscle spasm. She complains of no other joint symptomatology.
Her previous medical history is negative.
PHYSICAL EXAM
She was afebrile on presentation to the Alfred I. dupont Institute.
Physical examination demonstrated the following positive findings:
- Left hip 15 degrees abduction, 10 degrees addiction, 10 degrees external
rotation, 0 degrees internal rotation.
- Pain on range of motion, left hip
- Left lower extremity was 1.5 cm longer than the right lower extremity
- Antalgic gait
XRAYS
A CT scan in August showed joint effusion which was aspirated and evaluated.
The aspirate was negative for infection or other pathology.
An arthrogram performed was also negative. Both studies done at outside
facilities.
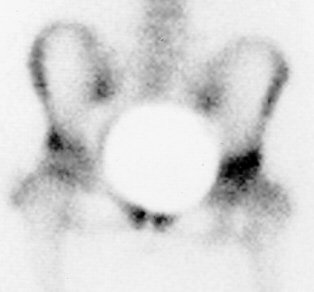
Recent radiographic findings revealed the following: Bone scan with
increased uptake left hip on both sides of joint .
Joint space narrowing left hip to 2 mm
.
Joint space narrowing left hip to 2 mm .
.
LAB VALUES
- PPD, HLA-B27, CBC with differential, Lyme panel, ANA -All within normal
limits.
- ESR mildly elevated at 31 mm/hr.
IDIOPATHIC CHRONDOLYSIS
Chondrolysis represents a process characterized by progressive destruction
of articular cartilage resulting in secondary joint space narrowing and
stiffness.
Types: May follow infection, trauma, prolonged immobilization and severe
burns about the lower extremities. Also, it may be a complication of slipped
capital femoral epiphysis.
Another type is idiopathic, characterized by an acute form of rapidly
progressive chondrolysis occurring most frequently during adolescence with
isolated involvement of the hip joint, but without a demonstrable cause.
HISTORY
Jones in 1971 described chondrolysis not associated with SCFE in black
adolescent girls. Since that time, reports of idiopathic scoliosis have
been recorded. As of 1989, after Daluga and Millar's study, 42 hips have
been recorded. The female to male ratio is 6:1 and 52% of these patients
are Caucasian.
ETIOLOGY
Etiology is unknown. Proposed theories include nutritional abnormalities,
mechanical injury, ischemia, abnormal intracapsular pressure, and an inherent
abnormal chondrocyte metabolism within the articular cartilage. The most
accepted theory is that proposed by Golding in 1973, which postulated articular
cartilage resorption to be secondary to an autoimmune response in genetically
susceptible individuals.
INCIDENCE
This remains unreported in the literature, although 42 have been reported
up to 1989. (Incidence of chondrolysis in SCFE is 8.2%).
CLINICAL PRESENTATION
- Adolescent girl average of 12.5 years.
- Right hip slightly higher than left hip
- Insidious onset of pain in anterior or medial side of affected hip
associated with joint stiffness and limp.
- Patient is afebrile
- Restriction of motion in all planes with associated muscle spasm
- Contracture about the joint; most commonly, fixed flexion, abduction
and external rotation
LABORATORY
CBC, UA, RF, ANA, HCA-B27, Blood culture, and TB (PPD) are WNL.
ESR can be slightly elevated and rarely over 30.
XRAYS
- Hallmark is narrowing of the joint space from normal 3-5 mm to values
<3 mm.
- Associated osteopenia of the periarticular osseous structures
- Irregular blurring of subchondral sclerotic lines
- Enlargement of the fovea capitis femori
- With time, can develop mild coxa magna and femoral neck widening and
frequently a premature closure of the proximal femoral physis and trochanteric
apophysis.
- Mild protrusion and a lateral buttressing osteophyte at the acetabulum
- Limited area of periosteal new bone formation along inferior femoral
neck
RADIOGRAPHIC TESTS INCLUDE
- Arthrography - help document cartilage resorption and joint space narrowing
- Bone scan shows increased uptake on both sides of joint
- CT Pelvis - document subchondral bone changes, cartilage resorption,
and narrowing of joint space
- MRI - may be of benefit, but there is no large volume of experience
using MRI found in the literature
PATHOLOGY
- Capsule is routinely thickened
- Lusterluss cartilage with irregular thinning, fibrillation and fragmentation
- Microscopic review of biopsy of synovium demonstrates nonspecific chronic
inflammation
DIFFERENTIAL DIAGNOSIS
- Infectious arthritis including TB: Will see increased CBC, ESR, Temp,
and positive PPD.
- Juvenile rheumatoid arthritis: There is an extended period of time
with symptoms prior to chondrolysis. Rarely see restrictions in range of
motion as that seen with Idiopathic Chondrolysis.
- Seronegative spondyloarthropathy: You will see additional joint involvement
and the HLAB-27 will be positive.
- Pigmented villonodular synovitis: Has a more chronic and prolonged
course. Usual findings include cystic erosions in subchondral bone and
a bloody aspirate.
TREATMENT
- Early recommended treatment included corrective osteotomy, bony fusion,
or joint arthroplasty.
- investigators proposed early and prolonged spica cast treatment until
fibrous ankylosis was achieved.
- investigators employed treatment protocol including therapeutic doses
- of NSAIDS, aggressive PT, periodic traction and bedrest, prolonged
non-weight, bearing or limited weightbearing, CPM.
- Current recommendations embrace philosophy of a more favorable long-term
prognosis for improved motion and function.
REFERENCES
- Bleck EE. Idiopathic chondrolysis of the hip. JBJS (AM) 1983;65:1266.
- Daluga DJ, Millar EA. Idiopathic chondrolysis of the hip. JPO 1989;9:405.
- Duncan JW, Nasca R, Schrantz J. Idiopathic chondrolysis of the hip.
JBJS (Am) 1979;61:1024.
- Duncan JW, Schrantz JL, Nasca RJ. The bizarre stiff hip-possible idiopathic
chondrolysis. JAMA 1975;231:382.
- Kozlowski K, Scougall J. Idiopathic chondrolysis-diagnostic difficulties.
Pediatr Radiol 1984;14:314.
- Lovell and Winter. Idiopathic chondrolysis of the hip. Pediatric Orthopedics
1037-1045.
 .
Joint space narrowing left hip to 2 mm
.
Joint space narrowing left hip to 2 mm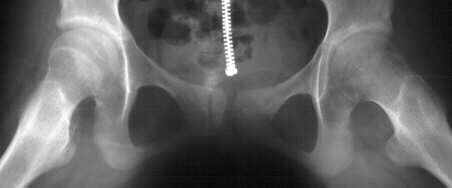 .
.