DEVELOPMENTAL COXA VARA
Eric Sandefur, D.O., Pediatric Orthopaedic Surgery
William G. Mackenzie, M.D., Attending Pediatric Orthopaedic Surgeon
August 2, 1995
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
DEFINITION :
- also known as cervical or infantile coxa vara
- represents coxa vara not present at birth but rather developing in
early childhood
- coxa vara is defined as any decrease in the femoral neck-shaft angle
less than 120 - 135 degrees
INCIDENCE :
- relatively uncommon, occurring approximately 1 in 25,000 live births
- occurrence is essentially equal in males to females and left to right
- bilateral involvement is note in 30 - 50% of patients
- recent reports have shown increase incidence in black population compared
with whites
- reports have also shown a familial pattern with an autosomal dominant
form of transmission
ETIOLOGY :
- currently remains unknown
- the most popular theory, proposed by Dylkkanes in 1960, states that
the deformity is caused by a defect of enchondral ossification of the femoral
neck. Weightbearing causes shearing stresses which result in fatigue of
the dystrophic one and progressive varus deformity results
- other proposed theories include:
- metabolic abnormalities cause a deficiency or delay in the ossification
process
- mechanical abnormalities may occur during development and early ambulation
- partial vascular insult to the inferior aspect of the femoral neck
- developmental abnormality which causes faulty cartilage formation and
maturation
- histologic studies have shown that there are abnormalities in both
cartilage production and metaphyseal bone formation. These findings are
similar to those found in the proximal tibia in patients with Blount's
disease.
CLINICAL PRESENTATION:
- most commonly seen between when the child begins to ambulate and age
six
- most common complaint is a progressive gait abnormality
- in unilateral involvement this is due to both abductor muscle weakness
and limb length inequality
- patients with bilateral involvement have a waddling gait and increased
lumbar lordosis (similar to that seen in bilateral DDH)
PHYSICAL EXAM:
- prominent and elevated greater trochanter
- positive Trendelenburg test
- limb-length inequality (usually less that 2.5 cm)
- decreased ROM with restrictions noted with abduction and internal rotation
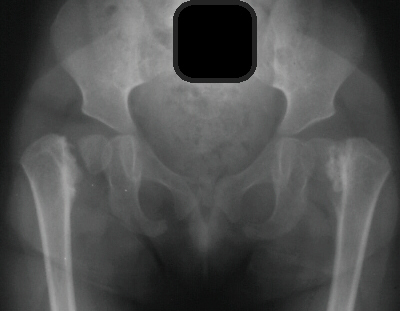
RADIOGRAPHIC FINDINGS:
- femoral-neck shaft angle below 90 degrees

- more vertical position of the epiphyseal plate with Hilgenreiner's-epiphyseal
angle greater than 40 degrees (normal is less than 25 degrees)
- triangular metaphyseal fragment in inferior femoral neck surrounded
by inverted Y (sine qua non)

TREATMENT :
aimed at the prevention of the secondary deformities caused by the disease's
natural history on the proximal femur
main objectives of surgical treatment include:
- correction of varus angulation

- changing of the loading characteristics from shear to compression of
the femoral neck
- restoring proper length of abductors muscles
- resolution of limb-length inequalities
current criteria for surgical intervention include one or more of
the following:
- femoral neck-shaft angle less than 90 - 100 degrees
- Hilgenreiner's-epiphyseal angle greater than 45 - 60 degrees
- documented decrease in the femoral neck-shaft angle
- Trendelenburg gait
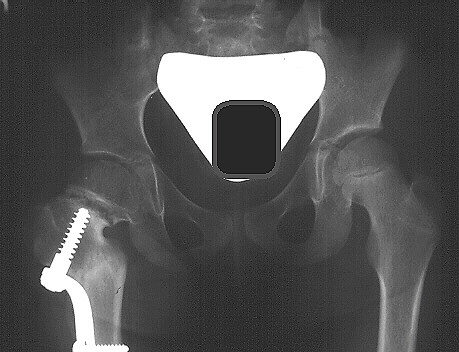
- currently, the most effective surgical treatment is a valgus producing
proximal femoral osteotomy (subtrochanteric vs intertrochanteric procedures
have similar results)
proper surgical treatment also includes:
- adductor tenotomy which allows for less forceful correction and improved
stability
- proximal femoral shortening osteotomy if necessary to help relieve
excessive femoral head pressure when the valgus angle is restored
- stable internal fixation and hip spica cast if needed
- goal of surgical treatment is to produce an overcorrection of valgus
angle to greater than 150 - 160 degrees, as well as, correction of epiphyseal
angle to less than 30 degrees
- The timing of surgery remains controversial. Several authors recommend
delay surgery until 5 6 years of age. Others state that surgery may be
performed after 18 months if the above criteria are met.
COMPLICATIONS:
- Recurrence of proximal femoral varus deformity-many feel that this
is due to undercorrection at surgery while others feel that it is due to
failure to place the osteocartilaginous defect into a compressive mode
- Premature physeal closure-the incidence may be as high as 89% and has
not been found to be related to physeal injury at the time of surgery
- Greater trochanteric overgrowth-associated with premature capital femoral
physeal closure and is commonly treated by greater trochanter transfer
or epiphysiodesis
- Acetabular dysplasia-found to be increase in patients with premature
physeal closure and inpatients who have had an undercorrection of the neck-shaft
angle less than 140 degrees
- other complications have included pseudarthrosis, avascular necrosis,
leg-length discrepancy, and degenerative arthritis
REFERENCES:
- Amstutz H.C. Developmental (infantile) Coxa Vara-a Distinct Entity.
Clin. Orthop. 72:242,1970
- Epps C.H. Jr. Current Concepts Review: Proximal Femoral Focal Deficiency.
J. Bone Joint Surg. 65A:867,1983
- Fisher R.L., Washkowitz W.J. Familial Developmental Coxa Vara. Clin.
Orthop. 86:2,1972
- Gaertner R.L. Developmental Coxa Vara: Observations on the Treatment
in This Infrequent Deformity. Orthop. 5:872,1982
- Pylkkanen P.V. Coxa Vara Infantum. Acta Orthop. Scand. 48:7,1960
- Schmidt T.L., Kalamchi A. The Fate of the Capital Femoral Physis and
Acetabular Development in Developmental Coxa Vara. J. Pediatr. Orthop.
2:534,1982
- Weighill F.J. The Treatment of Developmental Coxa Vara by Abduction
Subtrochanteric and Intertrochanteric Femoral Osteotomy with Special Reference
to the Role of Adductor Tenotomy.
- Clin. Orthop 116:116,1976
- Weinstein J.N., Kuo D.N., Millar E.A. Congenital Coxa Vara: A Retrospective
Review. J. Pediatr. Orthop. 4:70,1984