 .
On the T-2 weighted sequences there was abnormal increased signal of the
tibialis anterior, extensor digitorum longus and peroneus longus muscle
bellies suggesting atrophy
.
On the T-2 weighted sequences there was abnormal increased signal of the
tibialis anterior, extensor digitorum longus and peroneus longus muscle
bellies suggesting atrophyTHOM BROWN, MD, Resident, Orthopaedic Surgery
RICHARD KRUSE, DO, Attending, Pediatric Orthopaedic Surgery
KATRINA CONARD, MD, Attending, Pathology Department
March 18, 1996
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
A 2 and 5/12 year old white male presented to clinic with a 2-3 month history of limping on the right lower extremity. There was no history of trauma to the extremity, or a history of constitutional symptoms such as fever, chills, sweats, malaise or weight loss. Prenatal, perinatal and postnatal course were all normal.. The child was achieving all developmental milestones within expected age ranges.
Examination of the right lower extremity was significant for a distinct absence of ankle dorsiflexion and eversion activity to motor testing. Plantar flexion strength was graded as 5/5. Sensation was intact on the entire plantar aspect of the foot, with patchy sensation on the dorsum of the foot, including the first web space. A visible and audible foot slap was apparent while observing the child's gait. Examination of the knee revealed full range of motion without ligamentous instability. Quadriceps and hamstring strength were both 515 to motor testing. A discrete mass was palpable about the fibular head which was not mobile or pulsatile. There was no warmth, erythema or induration of the surrounding skin.
Radiographic examination of the left knee revealed no osseous abnormalities
![]()
![]() .
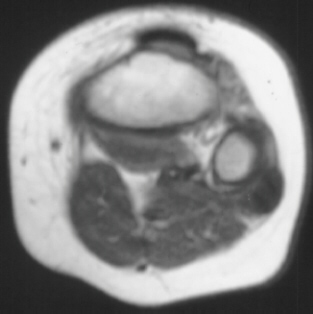
A fullness of the soft tissues was evident over the fibular head. MRI examination
of the left knee displayed a 2 cm. by 0.8 cm. lobulated mass in the region
of the common peroneal nerve with no enhancement
.
On the T-2 weighted sequences there was abnormal increased signal of the
tibialis anterior, extensor digitorum longus and peroneus longus muscle
bellies suggesting atrophy
.
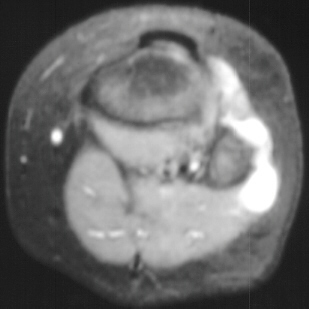
A fullness of the soft tissues was evident over the fibular head. MRI examination
of the left knee displayed a 2 cm. by 0.8 cm. lobulated mass in the region
of the common peroneal nerve with no enhancement
.
On the T-2 weighted sequences there was abnormal increased signal of the
tibialis anterior, extensor digitorum longus and peroneus longus muscle
bellies suggesting atrophy![]()
![]()
![]() .
EMG/NCS were performed which clearly documented electrodiagnostic evidence
of a severe peroneal neuropathy distal to the take-off of the nerve to
the short head of the biceps.
.
EMG/NCS were performed which clearly documented electrodiagnostic evidence
of a severe peroneal neuropathy distal to the take-off of the nerve to
the short head of the biceps.
The patient was placed in a molded ankle foot orthosis (MAFO) during the diagnostic work-up.
The differential diagnosis for this lesion included the following:
1) Neurilemmoma, 2) Neurofibroma, 3) Ganglion, 4) Hemangioma, 5) Neuroma.
Surgical exploration revealed a lobulated mass compressing and encompassing the peroneal nerve. The stalk of the cyst was found to be originating from the proximal tibio-fibular joint. All muscular and articular branches of the nerve were preserved during the ganglion excision. The stalk at the proximal tibio-fibular joint was transacted and left open.
Histopathological evaluation revealed a fibrous cyst wall without a discernible lining with adjacent and partially incorporated peripheral nerve.
The wound healed uneventfully. At three and a half months post-operatively, physical examination demonstrated some return of strength of the dorsiflexors and evertors (4/5) with the exception of the extensor hallucis muscle. Repeat EMG/NCS were postponed until clinical reevaluation 6 months post-operatively.
Ganglion cysts causing compressive peripheral neuropathies are an unusual, but when combined not an uncommon etiology. Ganglia are especially common in the region of the hand and wrist although they usually do not result in a compressive neuropathy. Several reports have been published documenting nerve compression in the upper extremity in the following locations: ulnar nerve in Guyon's canal, motor branch and cutaneous branch of the median nerve by a volar ganglion, and posterior interosseous nerve at the proximal radio-ulnar joint.
Peripheral nerve compression secondary to ganglion cysts in sites other than the upper extremity have been reported with increasing frequency probably because of improved imaging modalities. These locations include the tarsal tunnel and the posterior tibial nerve, the spino-glenoid notch and the suprascapular nerve and spinal nerve roots compressed by ganglion cysts arising from the facet joints.
The source and cause of ganglion cysts remains an unsettled issue. Fibrillar degeneration of collagen with accumulation of intra and extracellular mucin was previously thought to be the most plausible theory. This mechanism does not account for the self- limiting nature of cysts, their presence in children and adolescents, and their recurrence following aspiration or excision. Green believes that repetitive trauma or irritation results in the increased production of hyaluronic acid which subsequently dissects through the capsule or ligament to form the capsular ducts. These ducts and lakes coalesce to form the main subcutaneous cyst.
The microscopic appearance of ganglion cysts is conspicous for the absence
of inflammatory cells, lack of mitotic activity and the lack of a synovial
or epithelial lining of the single or multiloculated cysts. These cyst
walls are composed of compressed collagen fibers and occasional flattened
cells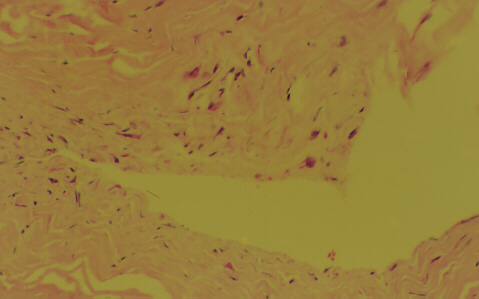 .
.
Non-operative treatment of historical interest includes rupture (Bible treatment), sclerosing solutions, hyaluronidase injection, and cross fixation with suture. All of these techniques have been abandoned secondary to failure/recurrence. Aspiration of the cyst followed by injection of lidocaine and steroids has proven useful in abating symptoms for variable periods of time. Surgical treatment remains the gold standard to which all other treatments are compared. Ganglion excision in all areas requires tourniquet control, meticulous hemostasis, excision of all mucinous pockets and careful preservation of surrounding neural structures.
In ganglion cysts compressing the peroneal nerve, few recurrences have been reported following surgical excision, even in cases where complete excision was not possible because of the risk of nerve damage.