DIASTROPHIC DYSPLASIA
Giuseppe Selva. M.D., Pediatric Orthopaedic Research Fellow
S. Jay Kumar, M.D., Attending, Orthopaedic Surgery
August 29, 1995
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
Diastrophic dwarfism is a rare skeletal dysplasia first defined by Maroteaux
and Lamy in 1960. More than 200 cases have been described in literature
(most from the U.S. and Finland).
The major clinical features of diastrophic dysplasia are:
- severe short-limb short stature
- cleft palate (27-59% of cases)
- typical ear deformity (cauliflower deformity in 85% of cases)
- progressive deformities and contractures of joints (100% of cases)
- progressive hip dysplasia (dysplasia 70% of cases; dislocation 22%
of cases)
- typical hand deformities (100% of cases)
- severe clubfoot (almost 100% of cases)
- progressive spinal curvatures (Lumbar lordosis 100% of cases, scoliosis
80% of cases)
- Early degenerative changes in joints (100% of cases)
Genetic features:
- Autosomic recessive transmission. ( D.T.D. and the McKusick type metaphyseal
chondrodysplasia are the only bone dysplasias with AR transmission).
- D.T.D. gene has been located on chromosome 5. (That excludes a primary
defect of IX collagen, whose gene maps on chromosome 6)
- 5-6% of cases due to new mutations.
- Prenatal diagnosis:
- In the first trimester through DNA analysis
- In the second trimester through US (short limb fetus with abnormal
metacarpophalangeal profile)
- Diagnosis at birth can be suspected because of the typical features.
- Phenotypic variants:
1. Lethal form (death soon after birth because of cardio- respiratory
insufficiency)
2. Diastrophic variant (mild form with only some features)
- Most patients have a normal life-span expectancy.
CLINICAL FINDINGS;
- Average length at birth: 33 cm
- Average adult height: 112 cm for both sexes (range 87 - 127 cm).
- Short-limb dwarfism, usually rizomelic (40%) or mesomelic (29%) .
- Puberal growth spur does not occur in these patients. Spinal deformities
and hip and knee contractures accentuate the apparent dwarfism.
- Nomocephalic head but typical facial appearance because of the squared
jaw, the narrow nasal bridge and the fullness of the circumoral area. These
children are been called "cherub dwarfs".
- Cleft palate in 27 to 59% of cases (lower frequency in diastrophic
variants and higher in lethal variants).
- Cauliflower ear deformity in 85% of typical DTDs and in 25% of diastrophic
variants. It occurs during the first 6 weeks of life after an acute inflammatory
process. Hearing impairment not usual (it is related to fusion of ossicles).
- Some patients present deformities of larynx and upper airways (laryngo
and tracheomalacia). They can develop severe respiratory insufficiency.
JOINTS:
The combination of marked limitation of motion of all major joints together
with a tendency to dislocation and subluxation characterize this disease.
Some authors believe there are 2 forms of DTD: the lax and the stiff type.
Virtually every joint is likely to develop stiffness. This is due to
the severe deformities of bones (epiphyseal and metaphyseal) as well as
soft tissue contractures.
Progressive dislocation of the hip, patella, radial head are often observed.
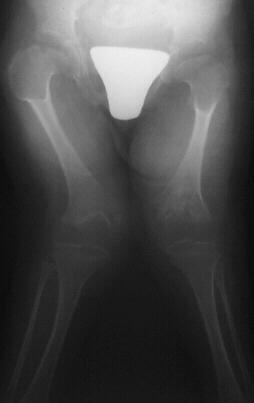
Hip dislocation and hip dysplasia have been reported, respectively
in 22% and 70% of patients. Delayed femoral head appearing, coxa valga
or, on the contrary, coxa vara are common findings. 
Valgus deformity of the knees, associated to flexion contracture,
is another common finding.
Clubfeet are another diagnostic feature occurring in almost every
patient. Clubfeet are usually very stiff and require surgical correction.
Particular findings are the adducted forefoot with a severe inward curvature
of the metatarsals  .
.
Hand deformities are essential for diagnosis and they are present
in almost 100% of cases. Hands are short and broad and deviated because
of the ulnar shortness. PIP joint stiffness is in contrasts with the hypermobility
of the thumb that is abducted over a short first metacarpal ("hitch-hiker"
deformity). 
Non-progressive lumbar lordosis is present in all patients and
it is probably related to flexion contractures of the hips. Cleft vertebral
laminae are common in both cervical and lumbar spine. Interpediculate narrowing
occurs in 75% of patients but spinal stenosis is unusual because pedicles
are not short, the posterior arch is relatively normal.
Scoliosis or kyphoscoliosis occur in 80% of patients. These curves
usually onset during the first 2 years of life and they are not due to
primary vertebral deformities. They must be carefully monitored because
of the potential progression (usually during adolescence). Most authors
suggest an aggressive orthotic treatment and early spine fusion.
Diastrophic dwarfs do not present atlo-axial instability or foramen
magnum stenosis. In some cases their C-spine develops progressive
kyphosis secondary to wedging of the lower cervical vertebrae. Progression
of this deformity can lead to neurologic deficits and death unless the
patient undergoes posterior or anterior and posterior spinal fusion.
The whole spine should be carefully monitored since the first year
of life.
RADIOGRAPHIC FINDINGS:
- Spine: generally the vertebral bodies are normal before the development
of spinal deformities. As previously mentioned, cleft laminae are common.
Deformities in C-spine vertebrae.

- Long bones: they are broad and short. Metaphyses are flared and expanded.
A chevron-like shape is often present in femoral and tibial metaphyses.
Epiphyseal centers appear late and are severely irregular and flat. Ulna
and fibula are usually short.
- Tubular bones in hands and feet are short and broad with typical deformities
in first metacarpal and in metatarsals
 .
.
DIFFERENTIAL DIAGNOSIS:
- Achondroplasia: no joint contractures (except elbows), no clubfeet,
hitchhiker thumb and ear deformities. Metaphyseal involvement (flared)
but epiphyses are normal. Skull involvement. Typical vertebral body deformities.
- Arthrogryposis: no dwarfism, no epi-metaphseal involvement, no ear
deformity and hitchhiker thumb
- SED: short-trunk dwarfism with stiff hips and often cleft palate
and clubfoot, but no thumb and ear involvement. Severe deformity of vertebral
bodies and epi-metaphyseal involvement of the proximal femur.
- Larsen syndrome: typical flat face, multiple joint dislocations present
at birth. Sometimes cleft palate, clubfeet and progressive cervical
spine kyphosis. No real dwarfism. No epi-metaphyseal abnormalities and
absence of the ear and thumb deformities.
TREATMENT:
Literature data are not enough to evaluate the orthopaedic treatment
of this disease.
Prevention and treatment of contractures, dislocations as well as spinal
and foot deformities should be the goal of the orthopedist.
CASE HISTORY:
O.A. female. DOB 2-6-91. Product of a normal gestation. Two healthy
half-sisters.
At birth:
- Disproportionate short-limb dwarfism with hitch-hiker thumbs
- Cleft palate (palatoplasty at age 1+1)
- Bilateral clubfoot (left worse right)
- Respiratory difficulties because of laryngomalacia
- Lack of extension in elbows and knees (moderate).
Walking age: 17 months (with some flexion of hips and knees)
Cauliflower deformity of ears occurred in the first weeks of life.
Cervical kyphosis with C3-C4 deformity and instability since first year
of life.
No neurologic involvement. Several MRIs (91-93) have shown no spinal cord
compression despite a somehow worsening of radiographs. 
Progressive genu valgum and increased flexion contractures of knees
and hips are now compromising the walking ability of the patient.
PREVIOUS ORTHOPAEDIC TREATMENT:
Feet: bilateral taping and serial casts. PMLR on the left foot (at age
9 months). Phelps braces. Feet are now plantigrade but with some residual
deformity.
ORTHOPAEDIC PLAN:
MRI C-spine. Hip arthrograms. Extension osteotomies for hip and knees.
REFERENCES:
- Beighton P. Inherited disorders of the skeleton. Ch. 2: 68-70. 2nd
ed. 1988
- Bethem D. et al. Disorders of the spine in diastrophic dysplasia. J.
Bone Joint Surg. 62-A: 529-536, 1980
- Gustavson K.H. et al. Lethal and non-lethal diastrophic dysplasia.
Clin. Genet. 28: 321-334. 1985
- Hollister D. W. et al. Diastrophic Dwarfism. Clin. Orthop. 114: 61-69,
1976
- Horton W.A. et al. The phenotipic variability of diastrophic dysplasia.
J. Pediatr. 93: 609-613, 1978
- Lovell and Winter's Pediatric Orthopaedics. Ch.4: The Osteochondrodysplasias.
3rd ed. 1990
- McKusick's Heritable disorders of connective tissue. Ch.14: 599-600,
5th ed. 1993
- Walker et al. Diastrophic dwarfism. Medicine, 51: 41-58; 1972
- Wynne-Davis/Hall/Apley Atlas of skeletal dysplasias. 258-273, 1985



 .
.