DISK HERNIATION IN CHILDREN AND ADOLESCENTS
DEAN HARTER, M.D., Resident, Orthopaedic Surgery
KIRK W. DABNEY, M.D., Attending, Pediatric Orthopaedic Surgery
April 3, 1996
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
Case History
This 17 year old white female was involved in an automobile accident.
She presented with localized low back pain and was diagnosed with lumbar
strain. Her pain increased despite maximum physical therapy.
At approximately 6 weeks post injury, she noted the onset of right leg
radiation in an S1 distribution. She also experienced occasional paresthesias
in the same area. Her LBP decreased at this point. She denied LE weakness
or bowel/bladder dysfunction.
Physical Examination
- decreased lumbar flexion
- Right list with forward bending
- no localized tenderness or spasm
- Straight Leg Raise test was positive at 45 degrees
- negative contralateral Straight Leg Raise test
- positive Lasegue's sign
- no focal neurological findings
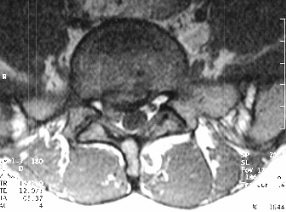
Radiological Evaluation
- plain x-rays normal, with mild spinal curve

- MRI-L5-S1 Right disc herniation with nerve root impingement

- Myleogram reveals nerve root impingement

Diagnosis and Treatment
- Right L5-S1 Disc Herniation
- L5-S1 Disc Herniation
Discussion
Incidence
- 1% of all surgically treated lumbar discs
- 7.8% in Japan
- M:F = overall
- age less than 12-greater in females
- most patients taller and heavier than average
Etiology
- trauma
- congenital spine anomalies
- familial predisposition
Congenital Spine Anomalies
- seen in 30% of patients
- transitional vertebrae
- spina bifida occulta
- congenital spinal stenosis
Familial Predisposition
- Varlotta JBJS 1973
- PTS age less than 16
- 92% positive family history
- 67% severe LBP
- 42% HNP
- risk for HNP prior to age 21-4-5 times greater with positive family
history
Symptoms
- severe LBP
- leg radiation
- often without leg pain at initial presentation
- time interval between LBP and onset of radiating leg pain-days to months
Symptoms
- back stiffness
- occasional paresthesias
- motor weakness, bowel/bladder dysfunction RARE
Physical Examination
- decreased back motion
- postural abnormality
- POSITIVE SLR
- HAMSTRING TIGHTNESS
- 50 % minor neurological abnormalities
Radiographic Findings
- mild nonstructural scoliosis
- loss of lumbar lordosis
- structural abnormality-30%
MRI
- current procedure of choice
- location same as adults
- disadvantage: MAY NOT PICK UP A SLIPPED VERTEBRAL APOPHYSIS
Differential Diagnosis
- slipped vertebral apophysis
- spondylolisthesis
- intraspinal tumor
- ankylosing spondylitis
- meningocele of the nerve root sheath
Treatment-Non operative
- bed rest
- heat/massage
- PT
- analgesics/muscle relaxants
- 40% response rate
- epidural steroids have not been studied in adolescents
Disc Excision-Indications
- failure of non-operative treatment
- progressive neurological deficit
Disc Excision
- no disc degeneration
- it is not necessary to remove the entire disc
- remove only the offending portion
Disc Excision-Results
- often immediate relief of symptoms
- long term results not as good
- Bradford
- 10 of 27 patients-intermittent back pain with long term f/u
- DeOrio
- 44 of 49 patients-excellent or good results,however,28 of those 44
later required tx for back pain
- 12 of 44 underwent a second operation
- O'Connell
- 91% cured or greatly improved
- 6 % reoperation rate
Slipped Verterbral Apophysis
- ring apophysis avulsion directly associated with a central disc herniation
- rare
- signs/symptoms similar to HNP
- majority located at L4-5 or L5-S1
- A single case of apophyseal fracture has been reported in the thoracic
spine(Geisinger Medical Center)
Ring Apophysis
- begins to ossify at approximately age 13
- fuses to the vertebral body at 17-18
- intervertebral disc is attached to the ring apophysis by Sharpey's
fibers
- fibrous attachments are stronger than the osteocartilaginous junction
Radiographic Evaluation
- plain x-rays-faint wedge shaped opacity seen on lateral in 50%
- CT-study of choice
- MRI
Treatment
- non-operative treatment almost always fails
- surgical excision of disc and associated fracture fragments is usually
needed
- bilateral laminotomies for adequate exposure
- excellent results with surgical treatment
References
- 1)Chapter 27 Weinstein, The Pediatric Spine 1994
- 2)Epstein Adolescent Disc Herniation Spine 9,4,427;1984
- 3)Epstein Limbus Lumbar Vertebral Fractures Spine 16,8,962;1991.
- 4)Gibson MRI of Adolescent Disc Herniation JBJS 69B,5,699;Nov 1987.
- 5)Bradford Lumbar Disc Herniations in Children and Adolescents Orthop
Clinics 2,2,583;July 1971
- 6)Zamani, MacEwen Herniation of the Lumbar Disc in Children and Adolescents
JPO 2,528;1982.
- 7)Harter, Hess Slipped Vertebral Apophysis of the Thoracic Spine: A
Case Report close personal communication with the author.