FACIOSCAPULOHUMERAL MUSCULAR DYSTROPHY
Eric Sandefur, D.O., Pediatric Orthopaedic Resident
William G. Mackenzie, M.D., Attending Pediatric Orthopaedic Surgeon
August 31, 1995
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY:
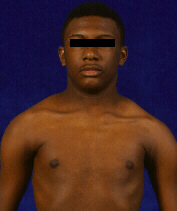
- HISTORY: 16 year old black male presented to the Alfred
I. duPont Institute with the chief complaint of left scapular winging
 and weakness of the left arm. Patient also complained to the inability
to abduct arms beyond the horizontal position.
and weakness of the left arm. Patient also complained to the inability
to abduct arms beyond the horizontal position.  Patients had also notice increasing atrophy of the left arm He was also
active in sports and played football but was unable to play basketball.
Patients had also notice increasing atrophy of the left arm He was also
active in sports and played football but was unable to play basketball.
- PHYSICAL EXAM: Facial characteristics included a transverse
smile, inability to purse lips or whistle, and unable to close his eyes
completely.
 Active abduction of the shoulders was approximately 90 degrees with a normal
passive ROM. Motor strength of (L) UE was 4/5 except deltoid which as 5/5.
Bother scapulae were elevated and medially rotated with marked winging
noted with attempted abduction
Active abduction of the shoulders was approximately 90 degrees with a normal
passive ROM. Motor strength of (L) UE was 4/5 except deltoid which as 5/5.
Bother scapulae were elevated and medially rotated with marked winging
noted with attempted abduction
- STUDIES: EMG/NCS revealed a myopathic process. Left deltoid muscle
biopsy revealed findings consistent with FSHD
- TREATMENT: Right Scapulothoracic arthrodesis with wiring ribs 3 - 6
and ICBG: June of 1994 Left Scapulothoracic arthrodesis with wiring ribs
3 - 6 and ICBG: June of 1995

- FOLLOW-UP: Markedly improve RPM with active abduction of 125 - 140
degrees and improved motor strength of both upper extremities.
ETIOLOGY/INCIDENCE:
- benign form of muscular dystrophy predominantly affecting muscles of
shoulder girdle and face
- autosomal dominate disorder
- there is considerable intrafamilial variability of phenotypic expression
- complete penetrance by fourth decade
- gene located at chromosome 4Q
- prevalence is 1 in 20,000
- occurs equally in male and female
ONSET:
- can present at any age bur most commonly occurs at end of 1st decade
or early second decade
- early onset FSHD is uncommon (<5%) but these children are typically
more affected and the disease process is more aggressive (children may
become confined to a wheelchair by age 8 - 9)
- life expectancy is normal
- disease progresses insidiously with prolonged periods of apparent rest
- partially affected or mild cases are common; some patients may not
realize the disease process is present
CHARACTERISTIC FEATURES:
- disease initially affects the face and shoulder girdle but later may
affect the trunk and pelvic girdle
1. FACIAL FEATURES:
- may be noted in infancy
- absent wrinkles from forehead and around eyes
- unable to close eyes properly (may sleep with eyes partially open)
- cannot whistle or purse lips; may have a transverse smile
- as the disease progresses, speech may become indistinct
2. SHOULDER GIRDLE FEATURES:
- main musculoskeletal problem is secondary to the weakness of should
girdle and scapular winging.
- due to marked weakness of the muscles that fix the scapula to the thoracic
wall, attempted abduction results in limited glenohumeral abduction with
marked winging of the scapula

- characteristic forward sloping to the shoulders
- horizontal position of clavicles d/t weight of UE and weakness of trapezius
- prominence of sternoclavicular joints
- there may be atrophy of biceps and triceps with normal forearm musculature
("Popeye forearm")
3. OTHER FEATURES:
- scoliosis and kyphoscoliosis are mild and usually occur late
- disease often accompanied by sensorineural hearing loss
- cardiac involvement is absent
- early involvement of tibialis anterior may be seen along with calf
pseudohypertrophy
LABS:
- CPK is usually normal
- histology: not impressive; most constant finding is isolated small
atrophic fibers intermixed with hypertrophic muscle fibers
TREATMENT:
- aim is to fix scapular winging and improve glenohumeral abduction
A. TECHNIQUES:
- Ketenjian (1978) described fasciodesis of scapula to the ribs utilizing
fascial trips, Mersilene tapes (preferred), or Dacron strips
- Copeland and Howard (1978) used cortical struts and screws to fix the
scapula to the ribs
- Bunch (1993) achieved fixation utilizing wires around the ribs and
passed through the body of the scapula
- Jakab and Gledhill (1993) modified Bunch's procedure and used wire
fixation only along medial border of scapula and ICBG
- Letournal (1990) passed a rib through a hole in the scapula and achieved
fixation with plates, screws, and wires
- all procedures resulted in improved abduction and flexion (Bunch and
Jakab and Gledhill had better abduction with their techniques averaging
125 - 140 degrees)
- also, the ability to sustain abduction and flexion was markedly improved
despite progressive generalized weakness
B. COMPLICATIONS:
- inappropriate positioning; there should be a 10 - 20 degree angle between
vertebral border of scapula and the spine. <30 degrees results in loss
of shoulder adduction and appearance of shrugging
- rib and scapula fractures
- brachial plexus palsy _+ brachial artery obstruction
- pneumothorax, pleural effusion, and pleuritic pain
- impaired pulmonary function (usually <10% of vital capacity)
- Pseudoarthrosis
REFERENCES:
- Bunch W.H., Siegel I.M. Scapulothoracic Arthrodesis in Facioscapulohumeral
Muscular Dystrophy. J. Bone Joint Surg. 75A:372-376,1993
- Copeland S.A., Howard R.C. Thoracoscapular Fusion for Facioscapulohumeral
Dystrophy. J. Bone Joint Surg. 60B:547-551,1978
- Drennan J.C. Neuromuscular Disorders. In Morrissey RT9ed), Lovell &
Winter's Pediatric Orthopaedics, Third Edition, 391-392,1990, Philadelphia,
JB Lippincott
- 4.Jakab E., Gledhill R.B. Simplified Technique for Scapulocostal Fusion
in Facioscapulohumeral Dystrophy. J. Pediatr. Orthop 13:749-751,1993
- Ketenjian A.Y. Scapulocostal Stabilization for Scapular Winging in
Facioscapulohumeral Muscular Dystrophy. J. Bone Joint Surg. 60A:476-480,1978
- Letournel E., Fardeau M., Lytle J.O., Sirrautl M., Gosselin R.A. Scapulothoracic
Arthrodesis for Patients Who Have Facioscapulohumeral Muscular Dystrophy.
J. Bone Joint Surg. 72A:78-84,1990
- Mackenzie W.G., Ishikawa S. Complications of Neuromuscular Disorders.
In Epp, Jr., CH & Bowen Jr., Complications in Pediatric Orthopaedic
Surgery, 627-630,1995
- Tachdjian M.O. Facioscapulohumeral Muscular Dystrophy. In Tachdjian,
MO(ed) Pediatric Orthopaedics, Second Edition, 2136,1990
 and weakness of the left arm. Patient also complained to the inability
to abduct arms beyond the horizontal position.
and weakness of the left arm. Patient also complained to the inability
to abduct arms beyond the horizontal position.  Patients had also notice increasing atrophy of the left arm He was also
active in sports and played football but was unable to play basketball.
Patients had also notice increasing atrophy of the left arm He was also
active in sports and played football but was unable to play basketball.