 and proximal right tibia
and proximal right tibia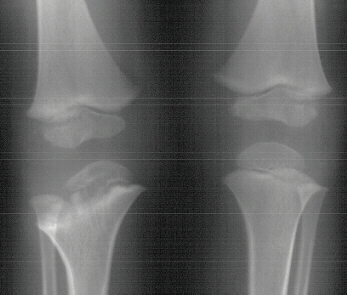 .
.
MAGDY ABDEL-MOTA'AL, M.D. , Orthopaedic Research Fellow .
WILLIAM MACKENZIE, M.D. , Pediatric Orthopaedic Surgery Attending .
March 12, 1996
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
Upper extremity limb length discrepancy is a rare occurrence. Although pediatric leg length equalization is well understood, surgical treatment of upper limb length discrepancy has rarely been described. This case report illustrates the use of Ilizarov's method for the treatment of humeral shortening secondary to septic neonatal growth arrest .
A three year one month old boy presented to AIDI with shortening of the right humerus. Clinical examination revealed 4 cm shortening of right arm and painless limitation of ROM of right shoulder; abduction was 150 degrees with 80 degrees at the glenohumeral joint and internal rotation was significantly limited. There was also 1 cm shortening of the right leg and a 10 degree valgus deformity of the same knee.
Radiological examination showed absence of proximal epiphysis of the
right humerus with marked deformity of the metaphyseal region. There was
mild shortening of the right tibia in association with destruction of the
lateral part of the proximal metaphysis and epiphysis. The diagnosis was
neonatal sepsis with multifocal osteomyelitis involving the right humerus
and proximal right tibia.
Xrays at age 11 show significant angualtion developed in the humerus
![]()
![]() .
However tibial growth was good
.
However tibial growth was good  .
.
At the age of 11 years 6 months the patient underwent corticotomy, application
of Ilizarov's external fixator and angular correction of right humerus.
A 5 mm EBI half-pin was placed in the proximal humerus laterally. Lateral
incision was placed over the distal humerus to identify the radial nerve;
a small incision was placed through the brachialis muscle down to the humerus
at the apex of the deformity for corticotomy. A significant amount of malrotation,
approximately 100 of the 150 degrees malrotation, was corrected by internally
rotating the distal fragment. A 1.8 mm Olive wire was drilled medial -to-lateral
across the distal fragment just above the olecranon fossa. The frame was
modified for 5/8`` ring with the open aspect anteriorly. It was placed
across the Olive wire and the arch was placed posterolaterally. The angular
correction devices were placed medially, and the lengthener was placed
laterally. An additional 5 mm half - pin was placed posteriorly to the
transfixion pin distally through the distal humerus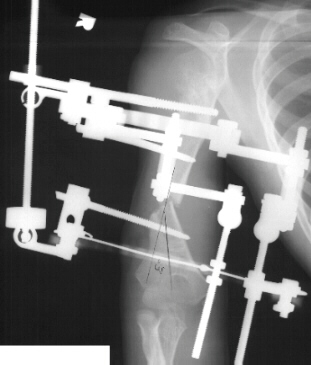 .
.
Lengthening started 7 days after the corticotomy with rate of 1 mm /
day. Nine weeks after the corticotomy there was good bone healing with
4 cm gap of new bone. ![]()
![]() A 30 degree of flexion contracture of the right elbow developed. Hardware
was removed and good new bone was noted
A 30 degree of flexion contracture of the right elbow developed. Hardware
was removed and good new bone was noted ![]() .
.
Partial hypoplasia of the upper limb with primary involvement of the humerus represents an infrequent pathological condition. However, it is always associated with considerable cosmetic and sometimes functional impairment.
The first case of humeral lengthening was reported by Dick and Tietjen in 1978. These authors treated a 2 and half year old boy affected by post-septic humeral hypoplasia of 4 cm, a Wagner apparatus was used in association with a shoulder spica with a window over the elbow . At the end of the lengthening, an AO plate and autogenous cortical and cancellous iliac bone grafts were applied through the original incision.
Another case was described by Olerud et.al. Their patient was a 20 year old man with a 12.5 cm shortening of the left humerus, most probably from destruction of the proximal humeral physis following septicemia in infancy. These authors used a vascularized fibular graft to fill the wide diastasis ( 12.5 cm ) reached during a lengthening process lasting 120 days The grafted arm was immobilized for 90 days with thoracobrachial appliance and Wagner device.
A third case of a 13 year one month old girl with 12.3 cm shortening of the left arm, was reported by Peterson. The etiology was not clear. There might have been a birth fracture or an infection ( either septic arthritis or osteomyelitis of the proximal humerus ) either in the newborn period or later. The patient underwent Wagner technique of osteotomy and gradual distraction. One hundred millimeters of length was obtained. Thirteen weeks after the original operation, the second stage surgery consisting of bone grafting, application of plate and screws and removal of the external lengthening device.
Humeral lengthening has also been used to correct arm length discrepancy secondary to different etiologic factors. Schopler presented a case of humeral lengthening for upper limb length discrepancy secondary to a unicameral bone cyst. Lamoureux reported a 10-year-old girl with idiopathic humerus varus. She underwent corrective osteotomy of the neck of the humerus followed by humeral lengthening. Cattaneo performed humeral lengthening in 4 patients with achondroplasia. He used Ilizarov's technique. Monte et. al. reported humeral lengthening in 6 extermities; the diagnosis was arthrogryposis 1, enchondromatosis 1, post-traumatic hypoplasia 2, and congenital humerus varus 2.
Monte summarized the causes of humeral hypoplasia as follows:
Peterson found that functional impairment was minimal with length discrepancy less than 6 cm that he limited the procedure to patients with discrepancy of more than 6 cm or to patients whose projected discrepancy at maturity would be more than 6 cm. He favored surgical lengthening over epiphyseal arrest of the contralateral normal proximal humeral physis.
Monte recommended humeral lengthening only when the length discrepancy was more than 3 cm., and that the lengthening should be limited to 30 % of the original length of the humerus . When longer lengthening is necessary, Monte advised to perform it in two stages at least two years apart, without exceeding 50% of the original length.
Three techniques exist for filling the bone defect created by gradual distraction after osteotomy: (A) Limb lengthening with cancellous bone graft and plating of the distracted gap. [ Wagner technique ] (B) Limb lengthening without bone grafting of the distraction gap.[ Ilizarov's technique ] and (C) Limb lengthening with cortical allograft of the distracted gap.
Ilizarov's technique entails external fixation of the bone with Kirschner wires of very small diameter. These can be easily removed in case of breakage or of local infection. They can be replaced under local anesthesia without interrupting the treatment.
Angular and rotational correction can be done simultaneously with the lengthening.