MASAFUMI HOMMA, M.D., Research Fellow of Orthopaedic Surgery
RICHARD W KRUSE, M.D., Attending Pediatric Orthopaedic Surgeon
October 4, 1995
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE.
In order to know what clinical and radiological features correlate to the ambulatory ability in osteogenesis imperfecta was retrospectively investigated.
Twenty four out of thirty two patients with the diagnosis of OSTEOGENESIS IMPERFECTA seen at Hamagumi Children's Rehabilitation Center between 1959 and 1990 were assessed. Age at first visit ranged from newborn to 33 years old, at an average of 8 years old. Age at latest visit ranged from10 to 48 years of old, at an average of 31 years old. Follow up term was 2 to 29 years, at an average of 19 years. Sixteen cases were male and 8 were female.
Family history, clinical findings: body height, blue sclera, dentinogenesis imperfecta, hearing disturbances, fractures in upper extremity, scoliosis, age of initial gate, age of onset of fracture, radiological findings: number of fractures, diameter of femur, and number of operation were investigated. The correlation between these factors and ambulatory status was also studied. Ambulatory status was classified into three groups (good: functional ambulator with or without orthosis and/or crutches, fair: wheelchair bound but able to stand or ambulate at home, poor: non-ambulator, wheel chair bound, unable to stand.)
A 18-years-old boy. Body height 114cm. Sillence type III.
The first visit was at 4 years of age. He sustained 16 fractures
in L/E and 30 fractures in U/E. He underwent 9 operations. He
had 80 degrees progressive scoliosis and recently underwent posterior
spinal fusion with internal instrumentation. He obtained his initial
gate at 18 months of age, and had been practical ambulator until
9 years old. However, the diameter of the femur which was 15mm
at 7 years of age![]() had started to decrease prior to the functional aggravation. He
eventually became a non-ambulator after the ankle joint fracture
at 9 years old.
had started to decrease prior to the functional aggravation. He
eventually became a non-ambulator after the ankle joint fracture
at 9 years old.![]() The diameter of the right and left femur at the age of 18
The diameter of the right and left femur at the age of 18 ![]() were
7 and 8 mm respectively.
were
7 and 8 mm respectively.
A 20-year-old -male. Body height 145cm. Sillence type I.
The first visit was 3 years of age. He sustained 12 fractures
in L/E and underwent 16 operations. He had no scoliosis. Initial
gate was obtained when he was 18 months old. He had been a practical
ambulator until 16 years old.![]() He can walk 100m on crutches, however, he rather depends upon
a wheelchair after he went to high school because of a fear of
fractures and convenience for quick transportation. The diameter
of the femur has been over 10 mm since 3 years old and is 17 mm
now.
He can walk 100m on crutches, however, he rather depends upon
a wheelchair after he went to high school because of a fear of
fractures and convenience for quick transportation. The diameter
of the femur has been over 10 mm since 3 years old and is 17 mm
now.![]()
A 14-years-old boy. Body height 124 cm. Sillence type sporadic.
The first visit was at 2 years-old. He sustained one fracture
in U/E and 8 fractures in L/E, underwent 10 operations, and has
60 degrees scoliosis. He became able to walk on crutches at 2
years old and had been a practical ambulator until 12 years old.
He sustained a fracture at the distal end of right femur where
an intramedullaly nail did not reached. He uses a wheelchair for
long distant transportation. This case is supposed to be on the
border line between ambulator and non-ambulator. The diameter
of the femur was 10 mm at 3 years of age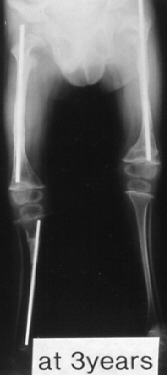 and 11mm at 13 years of age.
and 11mm at 13 years of age. ![]() No
increase of diameter has been observed despite rather thin intramedullaly
nailing.
No
increase of diameter has been observed despite rather thin intramedullaly
nailing.