ISCHEMIC NECROSIS AS A COMPLICATION IN DELVELOPMENTAL DYSPLASIA OF
THE HIP.
Carlos Cuevas De Alba, M.D., Pediatric Orthopaedic Research Fellow
S. Jay Kumar, M.D., Attending Pediatric Orthopaedic Surgeon.
August 30, 1995
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY:
This is an 11 months old white male patient who had congenital dislocation
of right hip. This was first detected 6 weeks of age. The patient was a breech child
delivered by C-section. He is the first child for this 38 year old mother.
At 6 weeks of age, he was placed in a Pavlik harness but this treatment
was unsuccessful. Closed reduction was performed, but the hip redislocated.
He was kept in an Ilfield brace for a short time and then had open reduction
followed by 3 months in a spica cast. Following removal of the cast he
redislocated again, and at that time the patient was referred to this Institute.
This was first detected 6 weeks of age. The patient was a breech child
delivered by C-section. He is the first child for this 38 year old mother.
At 6 weeks of age, he was placed in a Pavlik harness but this treatment
was unsuccessful. Closed reduction was performed, but the hip redislocated.
He was kept in an Ilfield brace for a short time and then had open reduction
followed by 3 months in a spica cast. Following removal of the cast he
redislocated again, and at that time the patient was referred to this Institute.
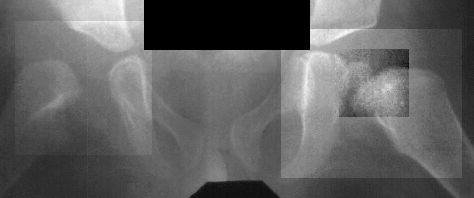
Physical exam showed the right hip to be dislocated. X-rays demonstrated
a dislocation of the right hip without the presence of an ossific nucleus
on the right side suggesting ischemic necrosis. Following traction, open reduction was repeated, with satisfactory results;
however subsequent radiographs show an irregular pattern of growth with
a tendency for subluxation even though it was treated part time in an abduction
brace.
Following traction, open reduction was repeated, with satisfactory results;
however subsequent radiographs show an irregular pattern of growth with
a tendency for subluxation even though it was treated part time in an abduction
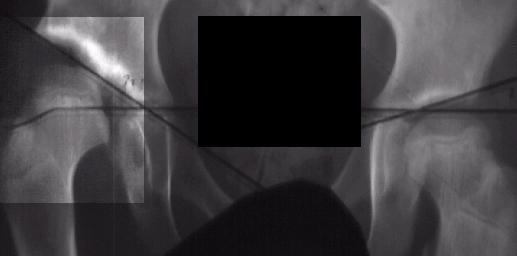
brace. X-rays
X-rays  and
arthrogram at two years of age show irregular ossification of the femoral
head and dysplastic acetabulum,
and
arthrogram at two years of age show irregular ossification of the femoral
head and dysplastic acetabulum, but the hip coverage was acceptable even in adduction.
but the hip coverage was acceptable even in adduction. At 5 + 8 years of age
At 5 + 8 years of age
 ,
a clinical diagnosis of Charcot-Marie-Tooth disease was made, and Shelf
arthroplasty was performed to increase the femoral head coverage.
,
a clinical diagnosis of Charcot-Marie-Tooth disease was made, and Shelf
arthroplasty was performed to increase the femoral head coverage. On the last evaluation (10 years old), the patient was pain free, and showed
acceptable range of motion, however, his right limb is 3 cms. short and
the patient is wearing a 2 cm. shoe lift.
On the last evaluation (10 years old), the patient was pain free, and showed
acceptable range of motion, however, his right limb is 3 cms. short and
the patient is wearing a 2 cm. shoe lift.
ISCHEMIC NECROSIS:
Ischemic necrosis of the proximal femur is an occlusion of a select
group of vessels that supply blood to the proximal femur. It is a serious
complication not observed in untreated hips; and it may occur in contralateral
normal hips after closed treatment. A non-ossified femoral head is more
susceptible to experience damage to the blood supply and subsequent necrosis
(14% versus 6% in ossified femoral head). Ischemic necrosis may affect
the ossific nucleus, with or without involvement of the epiphyseal growth
plate (partially or totally). This pathology may produce unsatisfactory
long term results, and the changes at maturity cannot be fully predicted
from the early changes seen in the femoral head.
Several factors have been attributed to either increase or decrease
the risk of ischemic necrosis of the proximal femur:
- - Excessive abduction. Compression of the medial circumflex artery
around the iliopsoas tendon increases the risk of Ischemic Necrosis
- - Reduction with inverted limbus.
- - Reduction position in non-reduced hip.
- + Prereduction traction decrease the incidence (34% to 4%).
- + Prereduction adductor tenotomy decrease the incidence of Ischemic
Necrosis reducing the excessive pressure of the femoral head.
- + Shortening of the femur as a part of treatment in walking age patients.
Recently, a detailed description of DDH in boys reported an increased
incidence of the redislocation, and ischemic necrosis of the proximal femur
in males more than in female patients:
TYPE OF TREATMENT BOYS GIRLS*
Success of Pavlik harness
0% 0%
Failure of Pavlik harness
7% I.N. 0-28% I.N
Close reduction 45% I.N.
6% I.N
Open reduction 73% I.N. 0-60%
I.N.
*Series including boys and
girls.
CRITERIA FOR DIAGNOSIS:
- Failure of appearance of the ossific nucleus during the first year
after reduction.
- Broadening of the femoral neck during the year after reduction.
- Increased radiographic density followed by fragmentation.
- Residual deformity after reossification is complete.
- Presence of persistent stiffness after cast removal even without radiological
criteria may be the earliest sign of Ischemic Necrosis
- GROUP II: Damage of the lateral aspect of the growth plate is
the principal characteristic of this group. X-rays show lateral physeal
bridge, and lateral metaphyseal notch or defect. Patients in this group
develop subcapital coxa valga with a tendency to have poor acetabular coverage.
- GROUP III: Damage of the physis with a large central defect.
Commonly, patients develop a short femoral neck without varus or valgus.
Relative "overgrowth" of the greater trochanter and limb length
discrepancy are the principal problems.
- GROUP IV: Damage of the entire femoral head and physis are characteristic
of this group. Irregular femoral head with varus, flattening, and coxa
magna. "Overgrowth" of the great trochanter, limb length inequality,
and subsequent early arthritis are the principal complications
TREATMENT RECOMMENDATIONS:
- Prevention and/ or correction of inadequate acetabular coverage.
- Improvement of trochanter-head relationship
- Management of leg length discrepancy
- Early detection and treatment of uncommon conditions associated with
ischemic necrosis (i.e. osteochondritis dissecans, chondrolysis)
TREATMENT ALGORITHM FOR AVASCULAR NECROSIS:
REFERENCES:
1. Borges J.L., Kumar S.J., Guille J.T. Congenital Dislocation of the
Hip in Boys. J. Bone Joint Surg. 77A:975-983,1995
2. Kalamchi A., MacEwen G.D. Avascular Necrosis Following Treatment
of Congenital Dislocation of the Hip. J. Bone Joint Surg. 62A:876-887,1980
3. O'Brien M.C., Millis M.B., Griffin P.P. The Early Identification
and Classification of Growth Disturbances of the Proximal End of the Femur.
J. Bone Joint Surg. 68A:970-980,1986
4. Thomas I.H., Dunnin A.J., Cole W.G., Menelaus M.B. Avascular necrosis
after Open Reduction for Congenital Dislocation of the Hip: Analysis of
Causative Factors and Natural History. J. Pediatr. Orthop. 9:525-531,1989
5. Jones D.A. Sub-capital Coxa Valga after Varus Osteotomy for Congenital
Dislocation of the Hip: A Report of Six Cases with a Minimum Follow-up
of Nine Years. J. Bone Joint Surg. 59B:152-158,1977
6. Mc Cluskey W.P., Bassett G.S., Mora-|Garcia G., MacEwen G.D. Treatment
of Failed Open Reduction for Congenital Dislocation of the Hip. J. Pediatr.
Orthop. 9:633-639,1989
7. Epps C.H., Bowen J.R. Complications in Pediatric Orthopaedic Surgery.
J. B. Lippincott Co., Philadelphia, 1995
8. Tachdjian M. Pediatric Orthopaedics. 2nd ed. Saunders, Co., Philadelphia,
1990
9. Kumar S.J., Marks H.G., Bowen J.R., MacEwen G.D. Hip Dysplasia Associated
with Charcot-Marie-Tooth Disease. J. Pediatr.. Orthop. 5:511-514,1985
<
 This was first detected 6 weeks of age. The patient was a breech child
delivered by C-section. He is the first child for this 38 year old mother.
At 6 weeks of age, he was placed in a Pavlik harness but this treatment
was unsuccessful. Closed reduction was performed, but the hip redislocated.
He was kept in an Ilfield brace for a short time and then had open reduction
followed by 3 months in a spica cast. Following removal of the cast he
redislocated again, and at that time the patient was referred to this Institute.
This was first detected 6 weeks of age. The patient was a breech child
delivered by C-section. He is the first child for this 38 year old mother.
At 6 weeks of age, he was placed in a Pavlik harness but this treatment
was unsuccessful. Closed reduction was performed, but the hip redislocated.
He was kept in an Ilfield brace for a short time and then had open reduction
followed by 3 months in a spica cast. Following removal of the cast he
redislocated again, and at that time the patient was referred to this Institute.