CONGENITAL KNEE DISLOCATION
MARTIN JENTER, D.O., Pediatric Orthopaedic Resident
J. RICHARD BOWEN, M.D., Attending Pediatric Orthopaedic Surgeon
February 28, 1996
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY:
HISTORY: A 29 week old gestation male presented with bilateral knee
dislocation, left hip subluxation, and right hip dislocation.
PHYSICAL EXAM: Right knee -30 to 20 degrees ROM, Left knee -20 to 20
degrees ; L. hip + Ortolani, R. hip - Ortolani
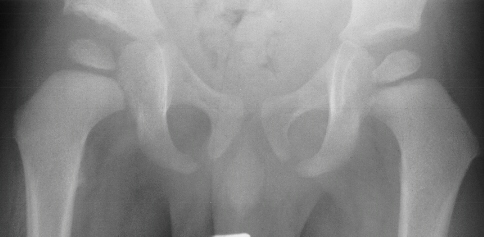
XRAYS: Reveal bilateral knee dislocations
 ,
and a left hip dislocation
,
and a left hip dislocation  .
.
TREATMENT: Manipulation, skin traction and splint for knees
Hips were placed in traction for 2 weeks full time, and 6 weeks part-time(
12hr/day). The right hip failed traction: than had an open reduction and
varus osteotomy at 1 year of age.
RESULT: ROM: R. knee 0-110 degrees, L. knee 0-120 degrees.; he started
ambulating 18 months with a well reduced femoral head  .
.
DISCUSSION:
per 100,000 general population; in Denmark 1% of DDH population
Female > Male 10:3 ratio, One-third bilateral, equal right and left
Environmental: Fetal position, increased in Breech
Fetal knee: round condyles, tibial plateau slope 35 degrees posterior
absence or hypoplasia of cruciate ligaments
quadriceps fibrosis acquired
Associated with Larson's syndrome
- Associated deformities:
- DDH in 45% of patients with CKD
- Foot deformity in 31%, clubfoot most common
- Elbow 10%
- Cleft palate, spina bifida, hydrocephalus, harelip, imperforate anus,
facial paralysis
- Also associated with: Arthrogryposis, myelodysplasia and Down's Syndrome
- Pathology:
- Quadriceps fibrosis and contracture
- Anterior subluxed tibia
- Hamstrings and ilio-tibial band anterior
- Absence suprapatellar pouch
- Underdeveloped or absent patella
- Hypoplastic or absent cruciates
- Grade I: minimum subluxation, knee 15-20 degrees. hyperextended, 45-90
degrees Flexion
- Grade II: displaced moderate, tibia anterior on femur, knee in 25-45
degrees hyperextension, flex to neutral
- Grade III: total displacement of tibia epiphysis, no contact, hip flexed,
foot at mandible
DIAGNOSIS:
1. Inspection, limited flexion
2. Ossification proximal tibia, distal femur hypoplastic or absent
3. Ultrasound: obliteration of suprapatellar pouch
TREATMENT:
- Early: Mild manipulation with flexion, cast, increase flexion at 2
week interval x 8wk.; Pavlik harness at night 2-3 months; Bi-valved splint
at night if lateral subluxation x 4-6 months
- Failed manipulation: Skin traction, prone, apply cast once 45-60 o
Flexion begin splinting once 100 o
- Failed skin traction: Reduction with K-wire distal femur, 2 wires in
tibia; femur traction anterior and proximal
Surgical treatment:
- Perform before weight bearing
- Ant-medial approach
- Inverted V in rectus femoris or tongue flap
- Medial and lateral parapatellar incision
- Free fibrosed quads, patella and tendons from bone
- Possible release anterior knee capsule, IT band and lateral septum
- Possible reconstruct cruciates if absent: semitendinosous for ACL
- Hip spica x 6 weeks, then night splint
RESULTS:
Nogi and MacEwen reviewed 27 knee dislocations (17 patients) without
associated syndromes
Results: No extensor lag
One patient with recurrent patella subluxation
Austwick and Dandy operated on three knees after 8 weeks casting, ROM
-45 to 45deg., ant-lat approach, tongue flap rectus, tight post cruciate
release, both patients walked age 18 months, all knees 0-120 degrees ROM.
Bell and Atkins treated 9 knees (5 children) operatively at average
9 months:
Technique: required splitting quads full length, slide to double length
V-Y flap. All patients had elongated ACL.
Immobilization in 40 o , further flexion causes skin tightening,
short tendoncast change at 3 weeks, flexion increased
20-30 o x 6 weeks, then free ROM.
Results: Extensor lag 30 o 8/9 knees, all patients walking
independently. One case skin necrosis due to skin tension: casted at 60
o
Conclusion: dislocation from either primary or secondary muscle imbalance.
Neuromuscular disease cause weak flexors, strong extensors: shorten quads.
Secondary cause: ant displaced hamstring with ant displaced tibia act as
extensors: short quadriceps result.
Johnson, Audell and Oppenheim reported on 23 knees in 17 patients:
- 12:5 Female to male, 4 premature birth, 7 breech, 7 clubfeet
- 10 knees improved conservatively in 3 months, ROM 3-94 o
- Normal ACL in 11/13 knees seen in surgery
- Operated group averaged 11-80 o motion
- Results: 8 good, 6 fair, 3 poor
- Use of arthrography to show loss of suprapatellar pouch
- prognostic for predicting need for surgery
- Best prognosis when treated non-operatively
Recommend: treat knee & foot before hip, do closed hip reduction
at time of open knee treatment; can maintain hip and knee reduction with
spica cast.
CONCLUSIONS:
The case presented here illustrates the success of non-operative treatment.
The patient exhibited several common findings for congenital knee dislocation
to include premature birth and associated hip dislocation. Skin traction
was used followed by splinting with resulting normal knee motion followed
by treatment of the hips. No complications resulted from this treatment
and the patient is a functional ambulator.
Surgery is planned for congenital knee dislocation when failure to progress
past 45 o flexion after 8 weeks or unable to reduce dislocation
by manipulation or traction. Patients needing surgery have poorer result.
REFERENCES:
- Austwick, D.H., Dandy, D.J. Early operation for congenital subluxation
of the knee. JPO 1983;3:85-7.
- Bell, M. J., Atkins, R.M., Sharrard, W.J.W. Irreducable congenital
dislocation of the knee. JBJS 1987;69-B,3:403-406.
- Johnson, E., Audell, R. Congenital dislocation of the knee. JPO 1987;7:194-200.
- Lovell and Winter. Pediatric Orthopedics. Lippincott Press, Philadelphia.
1990;vol 2:756-67.
- Nogi, J., MacEwen, D. Congenital dislocation of the knee. JPO 1982;2:509-513.
- Tachdjian, M. Pediatric Orthopedics. Saunders company, Philadelphia.
1990;vol 1:609-

 .
.
 .
.