PEDIATRIC ACUTE HEMATOGENOUS OSTEOMYELITIS
THOMAS KIM, MD, Orthopaedic Resident
J. RICHARD BOWEN, MD, Orthopaedic Attending
April 1, 1995
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY:
- Day of Admission to a hospital: this 9 month old male child had a history
of a normal pregnancy, delivery and growth. The mother noted a fever of
unkown origin for the previous 2 days with vague abdominal pain and diarrhea.
Initial workup revealed: temp 104, WBC 16,800 with left shift, CXray/Abd/Pelvis/Hip
Xrays negative, bone scan negative, spinal tap neg. The infant was admitted
with a diagnosis of viral infection vs. mycoplasma pneumonia. Started on
erythromycin.


- Hospital Day 2: Right hip was noted to be flexed and orthopaedic services
consulted. The right hip was aspirated, Gram stain: G PC, Started on Nafcillin
150mg IV q4. The child than had daily hip aspirations for decompression.
Final culture: coag (+) Staph aureus resistant to PCN.
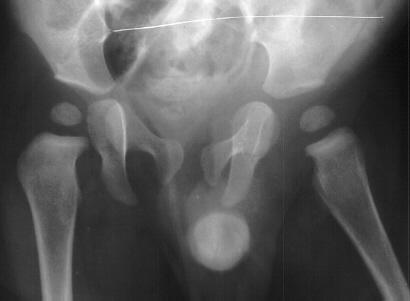
- Hospital Day 6: Respiked to 103.4. R hip Xray showed a defect in proximal
medial metaphysis, Possible osteomyelitis. The child was than taken to
the operating room for Incision & Drainage of Right hip via anterolateral
approach with suction irrigation system (seropurulent fluid drained).
- Post Operative Day 7: Drains removed. Respiked to 101.6. R hip Xray:
suggestion of demineralization of proximal metaphysis. The hip was reaspirated
and pus was obtained. Cultures neg.
- Post Operative Day 12: Respiked to 103.6. Gentamicin 1 mg IV q6 added
to Nafcillin. Daily aspirations of 10 cc purulent fluid, all cultures neg.

- Post Operative Day 18: R hip Xray: subluxation of R hip, possible metaphyseal
lucency consistent with osteomyelitis. Taken to OR for repeat I & D
of R hip via posterior approach with Penrose drains and hip spica cast
(15cc seropurulent fluid drained). Antibiotics changed to Oxacillin 225mg
IV q4.
- Post Operative Day 7: Drains removed. Afebrile.
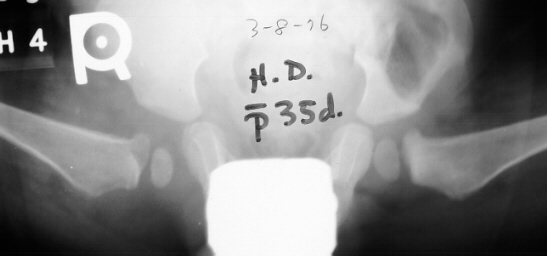
- Post Operative Day 9: Afebrile for 48hrs. Transferred to AI duPont
Institute. Initial labs: WBC 15,100, ESR 72. R hip Xray: changes in proximal
. metaphysis including lucency and demineralization, hip subluxated. Treated
with oxacillin and Pavlik harness.



- Hospital Day 12: WBC 12,600, ESR 48. Discharged home in Pavlik harness
x 1 yr., Oxacillin 250mg po q4.
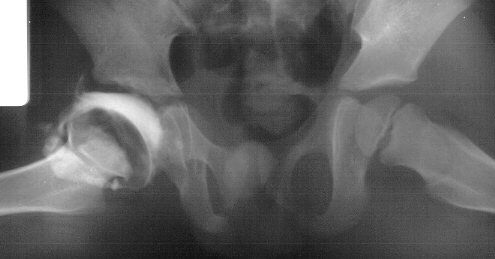
- 2 month Office Follow Up: Rt hip Xray: progressive destruction of capital
femoral epiphysis, cystic changes in metaphysis consistent with AVN.



- Age 6: Valgus osteotomy for subluxation and 2cm leg length inequality.






- Age 15: Valgus osteotomy for hip incongruity.



- Age 20: Hip arthroscopy. Hip fusion recommended.

Introduction
Before advent of antibiotics, acute hematogenous osteomyelitis had mortality
rate as high as 45%.
After introduction of PCN in 1944, mortality rate < 1 %.
No consistent peak incidence by age group.
Acute hematogenous osteomyelitis may coexistst with septic arthritis
especially in patients. < 12-18 months of age and in joints with intra-articular
metaphyses (eg. proximal humerus, proximal femur, distal lateral tibia,
proximal radius).
Pathogenesis
Risk factors: trauma (regional ischemia), bacteremia, illness, malnutrition,
immune system deficiency. Infection begins in metaphyseal venous sinusoid
(sluggish blood flow, poorly developed reticuloendothelial system).
Exudate exits porous metaphyseal cortex and forms subperiosteal abcess,
involucrum, sequestrum.
Evaluation and Diagnosis
HISTORY
- H/O recent or concurrent infection in 1/3 to 1/2 of cases.
- Unexplained bone pain and fever = osteomyelitis until proved otherwise.
LABS:
- WBC not invariably elevated (Scott et al: 41 % had WBC < 10,500).
- ESR elevated in majority of cases (not reliable in neonates, patients
with sickle cell anemia, lags behind clinical improvement).
- C-reactive protein (Unkila-Kallio et al: elevated in 98% of cases,
peak level on day 2, normal within a week of treatment).
- Blood cultures positive in 40 - 50% of cases.
XRAY:
- Early: deep soft tissue swelling only.
- Bone changes usually not present until > 1 week.
- Bone scans: Technetium-99m useful for localization in spine and pelvis,
detecting multiple sites of involvement.
- Not accurate in very early cases (< 24 hrs).
- Non specific (trauma, tumor, infection).
- False negative rate 4 - 20%.
- Bone aspiration does not affect results of bone scan if bone scan obtained
within 48 hrs after aspiration (Canale et al).
MRI:
- Sensitivity = bone scan
- Specificity > bone scan
ASPIRATION:
- Most valuable clinical test. Positive in 85-90% of cases.
- Neonates: group B Strop > Staph aureus
- Infants & children: Staph aureus (90% of cases)
- H. influenzae (6mo - 4yr)
- Sickle cell disease: Staph aureus > Salmonella
Treatment
Probable Initial
Patient Type Organism* Antibiotic
Neonates Group B Streptococcus, Cefotaxime, 100-120
Staphylococcus aureus, mg/kg of body weight
or Gram-negative rods for 24 hr, or oxacillin and
Hemophilus influenzae gentamicin, 5.0-7.5
mg/kg for 24 hr
Infants and S aureus (90% of cases) Oxacillin, lz-)o mg/kg for 24 hr
children
If allergic to Cefazolin, 100 mg/kg for 24 hr
penicillin
If allergic to Clindamycin, 25-40 mg/kc,
penicillin and for 24 hr, or vancomvcin,
cephalosporins 40 mg/kg for 24 hr
Patients with sickle S aureus or Salmonella Oxacillin and ampicillin
cell disease chloramphenicol or cefotaxime,
100-126 mg/kg for 24 hr
Duration of antibiotics: 6 weeks
Switch from IV to oral antibiotics once clinical response is seen (7
- 1 0 days).
Usual oral antibiotics: Dicioxacillin 50 mg/kg over 24 hr or Cephalexin
150 mg/kg over 24 hr
90% response rate to antibiotics alone when treatment is initiated within
first few days after onset of symptoms.
SURGICAL INDICATIONS:
- aspiration of pus (ie. abcess) sequestra in chronic osteomyelitis joint
sepsis
- delayed clinical response to antibiotics(> 36 hr)
Neonatal Osteomyelitis
Metaphyseal vessels penetrate directly into chondroepiphysis up to 12
- 18 mo.
Infections starting in metaphysis readily spread to chondroepiphysis
and joint.
Multiple sites involved in 40% (immature immune system).
This case is an example of untreated septic arthritis which caused avascular
necrosis of the proximal femur. The primary cause of this is undrained
septic hip. Repeated aspiration is not adequect treatment of a septic hip.
References
- Canale ST, Harkness RM, Thomas PA, et a[: Does aspiration of bones
and joints affect results of later bone scanning? J Pediatr Orthop 1985;5:23-26.
- Cole WG, Dalziel RE, Leitl S: Treatment of acute osteomyelitis in childhood.
J Bone Joint Surg Br 1982;64:218-223.
- Dormans JP, Drummond DS:. Pediatric Hematogenous Osteomyelitis: New
trends in presentation, diagnosis and treatment. J AAOS 1994;2/6: 333-341.
- Green NE, Edwards K: Bone and joint infections in children. Orthop
Clin North Am 1987;18(4):555-576.
- Jackson MA, Nelson JD: Etiology and medical management of acute suppurative
bone and joint infections in pediatric patients. J Pediatr Orthop 1982;2:313-323.
- Morissy RT: Bone and joint infections, in Morrissy Rt (ed): Lovell
and Winter's Pediatric Orthopaedics, 3rd ed. Phila: Lippincoft, 1990, vol
1, pp 539-561.
- Scoff RJ, Christofersen MR, Robertson WW Jr, et al: Acute osteomyelitis
in children: A review of 116 cases. J Pediatr Orthop 1990; 10:649-652.
- Unidia-Kallio L, Kallio MJT, Eskola J, et al: Serum C-reactive protein,
ESR, and WBC in acute hematogenous osteomyelitis of children. Pediatrics
1994;93:59-62.