PATELLAR DISLOCATIONS
DAVID J. ABRAHAM, MD Resident Orthopaedic Surgery
FREEMAN MILLER, M.D. Attending Pediatric Orthopaedic Surgeon
May 7, 1996
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY:
A 16 year old 220 pound black male was evaluated at the Sports Medicine
Clinic at AIDI 6 days after sustaining an acute injury to his right knee
while playing baseball. The patient related that he noticed acute onset
of R knee after striking out at bat. He heard a single clunk in his knee
and noticed immediate pain and swelling. He was evaluated at a local emergency
department and placed into a knee immobilizer and told to follow up in
Sports Medicine. He noticed that the knee "gave out" on him several
times since the accident.
On physical exam of the patient six days after injury the knee was noted
to have a large effusion. ROM was limited from 20 to 100 degrees of flexion.
There was significant medial retinacular tenderness with a mildly positive
apprehension test. His ACL, PCL, MCL and LCL ligaments were intact. McMurry's
test was negative, and his Q angle was 15 degrees.
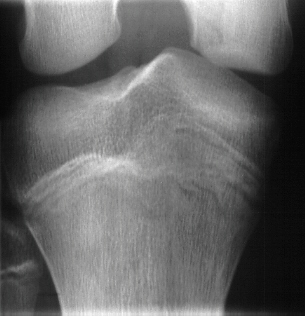
Radiographs revealed a large medial femoral defect and an intraarticular
calcification. 

 Based on these radiographs and his mechanical symptoms surgery was performed
for arthroscopic loose body excision. At arthroscopy the medial femoral
condylar defect was not apparent, but a large retinacular tear was discovered.
Also, the patient had an osteochondral fracture of the lateral femoral
condyle and a free 7mm by 5mm intraarticular cartilage fragment which was
removed.
Based on these radiographs and his mechanical symptoms surgery was performed
for arthroscopic loose body excision. At arthroscopy the medial femoral
condylar defect was not apparent, but a large retinacular tear was discovered.
Also, the patient had an osteochondral fracture of the lateral femoral
condyle and a free 7mm by 5mm intraarticular cartilage fragment which was
removed.
PATELLAR DISLOCATIONS:
- Most commonly due to twisting injury to knee.
- Only 10 % caused by direct trauma
- 24% incidence of positive family history of patellar dislocation
- Risk factors include:
- Shallow patellofemoral articular groove
- Patella alta
- Excessive Q angle
- Generalized ligamentous laxity
- Average age is 16- 20 years old, rare over 30
- Most common sports are football, basketball, baseball but not unusual
in gymnastics, simple falls, cheerleading or dancing.
- Female sex often associated with increased incidence of patellar dislocation
EVALUATION:
- Patient presents with a large, swollen knee held in a flexed position
with a prominent medial femoral condyle
- Reduced by gentle extension of the tibia, forceful medial pressure
on the patella is avoided. Often helpful to place the patient in the prone
position to extend the hip and relax the hamstrings.
- After reduction the patient has diffuse parapatellar tenderness and
often a palpable medial retinacular defect (vastus medialis insertion)
- Hemarthrosis can develop from the capsular tear and/or an osteochondral
fracture (usually the lateral femoral condyle or medial patella)
- Pre-reduction XR will often miss the OCD, bone fragments along the
medial patellar margin may be an avulsion fracture of the vastus insertion.
NONOPERATIVE TREATMENT:
- After reduction aspiration should be considered for a tense hemarthrosis,
blood checked for fat droplets indicating OCD
- Knee is placed in a knee immobilizer with lateral patellar pad to hold
patella in a reduced position Quad strengthening started as soon as possible
with straight leg raising.
- Natural history of nonoperativly treated patellar dislocations involve
recurrance in 1 in 6, minor residual symptoms in 2 of 6, and 3 of 6 will
be asymptomatic.(McManus, 1979.)
- The incidence of recurrant dislocation is decreases with age (Cash
and Hughston, 1987.)
14 year olds 60% redislocation
17-28 year olds 30 % redislocation
greater than 28 rare
OPERATIVE TREATMENT:
- Consider surgery for patients at high risk for recurrant dislocation:
- Risk factors:
- Osteochondral fracture of lateral femoral condyle
- age less than 14
- highly active/competative athlete
- palpable medial vastus defect
- contralateral evidence of dysplasia
- family history
- patella alta
- The role of lateral release in the treatment of recurrant dislocation
is controversial
- Metcalf reviewed 14 patients with recurrant dislocation and found 9
good, and 3 excellent results with 0 incidence of medial instability after
arthroscopic lateral release.
- Some feel that patients with obvious medial defect benefit from open
advancement of medial retinaculum and lateral release
- Patients with increased Q angle and ligament laxity may benefit from
distal realignment
- Roux-Goldthwait procedure involves splitting the patellar tendon and
medializing the lateral half (93% success)
- Hauser procedure transfers the patellar tendon and bony block of tibia
medially. (increased risk of developing OA secondary to increased joint
contact forces.)
- Elmslie Trillot Procedure-medially rotation a segment of ant. tibial
cortex including tibial tubercle
REFERENCES:
- Cash JD, Hughston JC. Treatment of acute patellar dislocation. Am J
Sports Med 1988; 16, 244.
- Larsen E. Conservative treatment of patellar dislocations. Clin Orthop
1982, 171:1321.
- McManus F, Rang M, Ahislin DJ. Acute dislocation of the patella in
children: the natural history. Clin Orthop 1979; 139, 88.
- Metcalf RW. An arthroscopic method of lateral release of the subluxating
or dislocating patella. Clin Orthop 1982: 167, 9.

 Based on these radiographs and his mechanical symptoms surgery was performed
for arthroscopic loose body excision. At arthroscopy the medial femoral
condylar defect was not apparent, but a large retinacular tear was discovered.
Also, the patient had an osteochondral fracture of the lateral femoral
condyle and a free 7mm by 5mm intraarticular cartilage fragment which was
removed.
Based on these radiographs and his mechanical symptoms surgery was performed
for arthroscopic loose body excision. At arthroscopy the medial femoral
condylar defect was not apparent, but a large retinacular tear was discovered.
Also, the patient had an osteochondral fracture of the lateral femoral
condyle and a free 7mm by 5mm intraarticular cartilage fragment which was
removed.