LUMBOSACRAL AGENESIS
Carlos Cuevas, M.D., Pediatric Orthopaedic Research Fellow
August 23, 1995
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
Lumbosacral agenesis is an uncommon condition characterized by absence
of different segments of lumbar spine along with total or partial absence
of the sacrum. The motor level can be correlated with the lowest vertebra
with pedicles, but sensory level could be above or below, and sometimes
asymmetric. Most the time, they have no bladder or bowel control.
ETIOLOGY:
- Unknown
- associated with maternal insulin-dependent diabetes (16% - 50%)
- failure of provocative mechanisms during early embryonic differentiation.
Freedman's theory (1950)
- inductive and formative influence of the spinal cord upon the vertebral
column. Detwiler's theory (1954)
- genetically determined exaggeration of the pattern of ontogenic cellular
death in mesodermal and neural elements of the posterior body regions.
Rosenthal (1968)
- inheritable genetic factors. Pouzet (1938)
CLINICAL FINDINGS:
Appearance:
Patient with multiple abnormalities with short trunk correlated with
the degree of lumbar agenesis; marked atrophy of the buttocks showing gluteal
dimples with short intergluteal fold, and horizontal anus. Characteristically
severe atrophy of the lower limbs with an appearance similar to that of
distal arthrogryposis; the lower extremities are in flexion, abduction,
and external rotation contracture at the level of the hips, and usually
there is a severe flexion contracture of the knees giving the classic Buddha-like
position often described. However, the appearance of the patient is directly
correlated with the degree of lumbosacral spinal involvement.
GENERAL FINDINGS:
- hydrocephalus: frequent when associated with myelomengocele
- myelomeningocele: occurs in 30 - 40%
- urinary tract: horseshoe kidney, solitary kidney, kidney malformations,
reflex and no bladder control are common
- inguinal hernia, imperforate anus, rectovaginal fistula, anal malformation,
Crohn's disease, no bowel control
- heart abnormalities are not common, but have been described
SPINE FINDINGS:
- cervical spine is commonly involved. Multiple vertebral fusions, C2
- C3 fusion
 ,
odontoid abnormalities, odontoid absence, and ball and socket occiput-atlanto
joint with
,
odontoid abnormalities, odontoid absence, and ball and socket occiput-atlanto
joint with  or
without instability
or
without instability
- segmentation or formation defects are common findings in vertebrae
and ribs of patients with sacral agenesis
- scoliosis is better correlated with the presence of thoracic or thoracolumbar
vertebrae abnormalities (i.e. hemivertebra) than the lumbosacral defect.
However, scoliosis may occur when an asymmetrical spino-pelvic "joint"
is seen, or a part of the sacrum remains in the pelvis
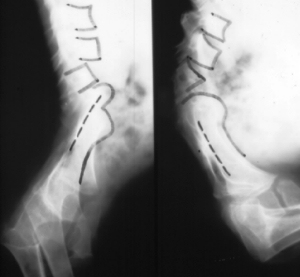
- kyphosis is common finding, it's correlated with high level lumbosacral
agenesis and spino-pelvic instability. Kyphosis is often severe, reducing
the abdominal capacity and producing rib-pelvic "pseudo-joint"

LOWER EXTREMITIES:
- frequently, hips have a flexion, abduction and external rotation contracture.
Sometimes, the hips are dislocated secondary to pelvic obliquity and/or
the acetabula reorientation

- commonly, the knees have a flexion contracture, and sometimes this
is severe
- feet: plano-valgus, calcaneo-valgus, vertical tali, and tarsal and
metatarsal synostosis, are frequent findings in patients with lumbosacral
agenesis.
CLASSIFICATION:
Renshaw (1978) classified sacral agenesis in four types:
- Type I: total or partial unilateral sacral agenesis
- Type II: partial sacral agenesis with a partial but bilaterally symmetrical
defect and a stable articulation between the ilia and a normal or hypoplastic
first sacral vertebra (most common).
- Type III: variable lumbar and total sacral agenesis with the ilia articulating
with the sides of the lowest vertebra present
- Type IV: variable lumbar and a total sacral agenesis, the caudal end-plate
of the lowest vertebra resting above either fused ilia or an iliac amphiarthrosis
TREATMENT:
Extensive investigation of the whole spine; the genitourinary, cardiovascular,
and gastrointestinal tracts should be done in the initial approach of patients
with lumbosacral agenesis.
Three major trends of management have been described:
- Ablation of the lower extremities (subtrochanteric level or knee disarticulation)
plus prosthetic fitting (Russel, 1963; Aiken et al, 1967; Tachdjian, 1990)
- Spinal pelvic fusion: "increase abdominal capacity, and protect
viscera from unphysiologic compression" (Winter, 1991, Renshaw, 1978)
- Correction of the inferior limb deformities and orthotic fitting; based
on the fact that most patients have preserved protective sensation and
proprioception of the lower extremities. "Spinal-pelvic motion is
helpful to maintain the sitting position in patients with fixed flexion
contracture of the hips". (Banta, 1969; Andrish, Kalamchi, and MacEwen,
1979)
HIP:
- Early open reduction may be indicated; some times secondary procedures
including varus derotational osteotomy with or without pelvic osteotomy
may be required
- In a fixed flexion contraction deformity of the hip, extension proximal
femoral osteotomy may be indicated.
KNEE:
- Posterior release and sometimes distal femoral flexion osteotomies
may be indicated to increase the extension of the knees (Recurrence of
the deformity in the absence of quadriceps motion may occur).
FOOT:
- Plantigrade foot is the goal of the treatment; usually surgical releases
in early age are indicated and orthotic support is needed to avoid recurrence
of the deformities, and permit adequate weight-bearing in ambulatory patients.
REFERENCE:
1. Andrish J., Kalamchi A, MacEwen, G.D. Sacral Agenesis: A Clinical
Evaluation of the Management, heredity and associated anomalies. Clin.
Orthop. 139:52-57,1979
2. Banta J.V., Nichols O. Sacral Agenesis. J. Bone Joint Surg. 51:693-703,1969
3. Dumont C.E., Damsin J.P., Forlin E., Carlioz H. Lumbosacral Agenesis.
Spine 18:1229-1235,1993
4. Renshaw T.S. Sacral Agenesis. The Pediatric Spine - Principles and
Practice. 1:2214,1994,
Raven Press, New York
5. Phillips W.A. Sacral Agenesis. Spine - Principles and Practice. 1:2214,1994,
Raven Press, New York
6. Jay Kumar S. Personal Communication. July 1995
7. Phillips W.A., Cooperman D.R., Linquist R.C., Sullivan R.C., Millar
E.A. Orthopaedic Management of Lumbosacral Agenesis. Long Term Follow Up.
J. Bone Joint Surg. 64A:1282-1294,1982
 ,
odontoid abnormalities, odontoid absence, and ball and socket occiput-atlanto
joint with
,
odontoid abnormalities, odontoid absence, and ball and socket occiput-atlanto
joint with  or
without instability
or
without instability