SKEWFOOT
CHARLES J. ODGERS, M.D., Resident, Orthopaedic Surgery
ROBERT P. STANTON, M.D., Attending Pediatric Orthopaedic Surgeon
April 10, 1996
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY:
A 2+1 year-old boy was seen at A.I. duPont Institute for evaluation
of intoeing. He had been previously diagnosed with bilateral metatarsus
adductus at another institution. His prior treatment consisted of serial
casting for eight weeks begun shortly after birth, followed by corrective
shoes until age 12 months. His parents felt that the metatarsus adductus
had improved since birth, however they still had concerns over the residual
deformity. They denied that their child had any functional problems. There
was a positive maternal family history of "intoeing" which was
treated with a Dennis Browne bar and corrective shoes.
Initial Exam
Examination revealed a well-appearing child. He had bilateral mild internal
tibial torsion, however the major component of his intoeing appeared to
be secondary to bilateral metatarsus adductus deformities which were supple
and flexible and they were both able to be corrected to neutral position.
Disposition
The patient did not have x-rays of his feet at this time. The working
diagnosis remained metatarsus adductus, and the patient was recommended
to wear straight last shoes to see if that would obtain further correction.
He was told to return in six months at which time AP and lateral x-rays
of both feet would be obtained .
.
Follow-up
The patient returned for follow-up, now 5+1 years-old. His mother stated
that he still had residual intoeing, and he appeared more clumsy with gait
than other children his age. She was concerned that his metatarsus adductus
had not corrected, and she wanted to know if anything more could be done.
The patient still had not had any functional problems, nor had he any shoewear
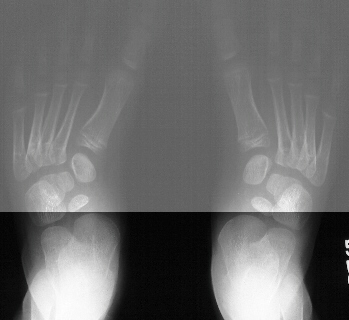
problems. Examination revealed bilateral flexible metatarsus adductus deformities.
There was no evidence of any skin breakdown or callous formation. He did
have a noticeable valgus right heel with a less obvious left heel valgus
deformity. His subtalar motion was maintained. AP and lateral standing
radiographs were obtained.
SKEWFOOT
Introduction
- Rare complex foot deformity of malalignment of the tarsals and metatarsals
- Recognized clinically by forefoot adduction and hindfoot valgus
- Originally coined by McCormick and Blount in 1949
- Synonyms include S-shaped foot , serpentine foot, and Z-foot deformity
- Never been recorded at birth- often discovered after cast treatment
for metatarsus adductus or clubfoot
- Problem- Many unknown variables with this condition including the definition,
prevalence, etiology, natural history , and treatment
Definition
- Inconsistent terminology
- 1933- Peabody and Muro - labeled foot shape congenital metatarsus varus
and differentiated it from more common and benign congenital metatarsus
adductus
- 1949- McCormick and Blount- used skewfoot to describe a group of foot
deformities including metatarsus adductus, metatarsus varus, metatarsus
adductovarus, and metatarsus adductocavovarus
- 1950- Kite- identified nine feet in series of 300 with benign forefoot
adduction characterized by severe forefoot adduction and fixed heel valgus
angulation which were very resistant to treatment- called them metatarsus
adductus and later renamed serpentine metatarsus adductus
Clinical Features
- Presenting complaints- most often shoewear and abnormal gait
- Forefoot adducted and increased heel valgus( +/- Achilles tendon contracture)
- Can develop painful callosities and bursa
Radiographic Evaluation
- No universally accepted clinical or radiographic criteria for defining
relationships of forefoot and hindfoot in flatfoot, skewfoot, or metatarsus
adductus- how much forefoot adduction needed to reclassify flatfoot as
skewfoot?
- 1986-Berg- first attempt to classify metatarsus adductus and skewfoot
radiographically- many faults of study
- Radiographs of children from two to seventeen months of age when bone
ossification is limited and irregular
- Made gross assumptions regarding position of unossified navicular,
a key element in his classification system
- Cook et al.- found large inter- and intraobserver disagreement using
this classification system
- Medial angulation of the talus-1st metatarsal line - indicative
of forefoot adduction
- Increased Kite's talocalcaneal angles on AP(>35) and lateral(>45)-
indicative of hindfoot valgus
- Lateral subluxation of navicular bone on talus
Etiology-unknown
- Early authors believed skewfoot resulted from improper use of cast
in attempt to correct clubfoot and metatarsus adductus deformities
- Peabody and Muro- muscle balance resulting from variation in the insertion
of the tibialis anterior
Natural History- unknown
- Do some patients have spontaneous correction with time as with metatarsus
adductus and flexible flatfoot?
- Prevalence of long term disability?
- Fact- some patients clearly have pain, callosities, and difficulty
wearing shoes as early as 1st decade
Treatment
- Role of manipulations and serial casting- consider only if discovered
during infancy
- Symptomatic non-operative treatment- modifications in shoewear
- Surgical treatment- Indicated in older patients who have failed conservative
treatment- most suggestions have been based on theory- need to correct
all components of deformity
- Peterson - combined tarsometatarsal capsulotomies with concurrent Grice
subtalar arthrodesis- good result however only three patients
- Coleman- proposed medial cuneiform opening-wedge osteotomy with plantar
fasciotomy- does not address hindfoot deformity
- Mosca-Used combination of calcaneal lengthening osteotomy(modified
Evan's technique), medial cuneiform opening wedge osteotomy, and Achilles
lengthening- 9 of 10 satisfactory results- technique preserves motion of
all joints- only short term follow-up
REFERENCES:
- Berg E: A reappraisal of metatarsus adductus and skewfoot. J. Bone
and Joint Surg., 68-A:1195-1196, Oct. 1986.
- Coleman S: Complex Foot Deformities in Children, pp. 267-272. Philadelphia,
Lea and Febiger, 1983.
- Kite J: Congenital metatarsus varus. Report of 300 cases. J. Bone and
Joint Surg., 32-A: 500-506, July 1950.
- McCormick D, and Blount W: Metatarsus adductovarus. "Skewfoot".
J. Am. Med. Assn., 141:449-453, 1949.
- Mosca V: Calcaneal lengthening for valgus deformity of the hindfoot.
Results in children who had severe, symptomatic flatfoot and skewfoot.
J. Bone and Joint Surg., 77-A:500-512, April 1995.
- Peabody C, and Muro F: Congenital metatarsus varus. J. Bone and Joint
Surg., 15:171-189, Jan. 1933.
- Peterson H: Skewfoot(forefoot adduction and heel valgus). J. Pediat.
Orthop., 6:24-30, 1986.
 .
.