SOFT TISSUE SURGERY AS A PROPHYLACTIC MANAGEMENT
OF THE SUBLUXATION AND DISLOCATION OF THE HIP IN CEREBRAL PALSY
MASAFUMI HOMMA, M.D.,D.M.Sc, Research Fellow of Orthopaedic Surgery
KIRK W. DABNEY, M.D., Attending of Pediatric Orthopaedic Surgery
December 5, 1995
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY
PATIENT 1:
An eight year old female with spastic diplegiapresented with no mental
retardation and she has been an ambulator since her five years of age.
She was the 3 pound 5 ounce product of a 30 week gestation which was complicated
by a low birth weight and respiratory distress at birth. Sitting alone:
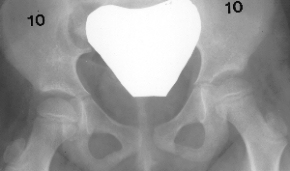
11m.. Crawling: 2y.+6m.. At 2y. + 3m., an initial X-ray showed a migration
index of the right hip of 30% and the left hip 50%. Hip abduction was 50 degrees and popliteal angle was 10 degrees bilaterally.
In the prone position with her hips extended, she has 60 degrees of internal
rotation bilaterally and 40 degrees of external rotation on the right and
60 degrees of external rotation on the left. She had a negative Thomas
test bilaterally. At 2y.+6m., bilateral iliopsoas release, bilateral
adductor longus and gracilis release were performed. At 4y.+ 2m., she
could ambulate with a walker. Hip abduction was 60 degrees bilaterally.
Popliteal angle was 30 degrees bilaterally, x-ray showed normal hips.
Hip abduction was 50 degrees and popliteal angle was 10 degrees bilaterally.
In the prone position with her hips extended, she has 60 degrees of internal
rotation bilaterally and 40 degrees of external rotation on the right and
60 degrees of external rotation on the left. She had a negative Thomas
test bilaterally. At 2y.+6m., bilateral iliopsoas release, bilateral
adductor longus and gracilis release were performed. At 4y.+ 2m., she
could ambulate with a walker. Hip abduction was 60 degrees bilaterally.
Popliteal angle was 30 degrees bilaterally, x-ray showed normal hips. At 7y.+5m., she underwent bilateral distal hamstring lengthening , rectus
femoris transfer, gastrocnemius recession, and bilateral. lateral column
lengthenings for her crouched gait and valgus foot deformities. Recent
popliteal angles were 25 bilaterally, Thomas test 15 bilaterally, and hip
flexion and abduction were all normal. Six years after adductor lengthening
both hips are normal.
At 7y.+5m., she underwent bilateral distal hamstring lengthening , rectus
femoris transfer, gastrocnemius recession, and bilateral. lateral column
lengthenings for her crouched gait and valgus foot deformities. Recent
popliteal angles were 25 bilaterally, Thomas test 15 bilaterally, and hip
flexion and abduction were all normal. Six years after adductor lengthening
both hips are normal.
PATIENT 2:
A six year old boy presents with mental retardation and spastic quadriplegia.
He is a non-ambulator who was delivered by C-section at 31-weeks gestation
of a twin pregnancy. Body weight at birth was 1558 gram. Social smile:
5 mo.. Physical therapy was started from 6th month. Turning over: still
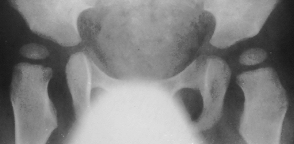
not possible. Sitting: still unstable. At 2y.+4m., the slight subluxation
of the right hip was noticed. Thomas was 30 degrees and abduction was 15 degrees bilaterally. At 4 y.o.,
the subluxation progressed on x-ray.
Thomas was 30 degrees and abduction was 15 degrees bilaterally. At 4 y.o.,
the subluxation progressed on x-ray. Popleteal angle was 45 degrees and Thomas was 30 degrees bilaterally.
At 4y.+1m., he underwent soft tissue release:fractional lengthening
of proximal part of semitendinosus and biceps ; slide lengthening of semimembranosus;
tenotomy of adductor longus and Gracilis and psoas major; fractional lengthening
of rectus femoris and intermedius. An abduction pillow has been applied
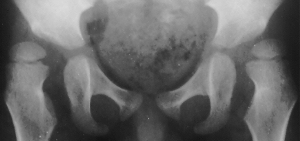
post-operatively. At 6 y.+ 2m. (post-op. 2y.), flex; 140 degrees, abd;
35 degrees,p-angle; 35 degrees bilaterally,Thomas; 10 degrees on the right
and 15 degrees on the left;. The x-ray showed dramatical improvement of
the subluxation and acetabular coverage.
Popleteal angle was 45 degrees and Thomas was 30 degrees bilaterally.
At 4y.+1m., he underwent soft tissue release:fractional lengthening
of proximal part of semitendinosus and biceps ; slide lengthening of semimembranosus;
tenotomy of adductor longus and Gracilis and psoas major; fractional lengthening
of rectus femoris and intermedius. An abduction pillow has been applied
post-operatively. At 6 y.+ 2m. (post-op. 2y.), flex; 140 degrees, abd;
35 degrees,p-angle; 35 degrees bilaterally,Thomas; 10 degrees on the right
and 15 degrees on the left;. The x-ray showed dramatical improvement of
the subluxation and acetabular coverage.
Prevalence:
- The prevalence of hip subluxation and dislocation in cerebral palsy
varies from 2.6 to 28 per cent (25-30% in large series).
- Dislocation of the hip occurs more frequently in the non-ambulatory
patient with the spastic quadriplegia. It is rare in the hemiplegic.
Pathogenesis:
- Acetabular dysplasia is absent in early stages of dislocation.
- Paralytic dislocation of the hip usually develops late in childhood
at around five to seven years of age.
The following factors lead to dislocation of the hip in cerebral palsy:
- The adductors, flexors, and medial hamstrings are relatively overactive
compared with their antagonists. This leads to an adducted, flexed, internally
rotated hip which tends to dislocate posteriorly.
- Secondary femoral antetorsion and acetabular insufficiency.
- Mental retardation, the retention of neonatal reflexes, and total involvement
of the body indicates an increased likelihood of hip dislocation.
- Scoliosis and hip dislocation are often observed in combination. There
is a debate about the temporal relationship between scoliosis, pelvic obliquity
and hip dislocation.
Clinical features of subluxation:
- The patient may have the progressive limitation of hip abduction and
progressive flexion contracture. The popliteal angle may be deteriorated.
- Hip joint may be painful.
Clinical features of dislocation:
- Marked limitation of hip abduction. In the ambulatory patient, walking
may be impaired. Sitting balance is impaired. Scoliosis develops.
Radiographic features:
- Subluxation is sometimes detected only by X-rays.
- Widening of the medial joint space is the earliest sign. Shenton's
line will be broken.
- With persistence of subluxation or dislocation, posterior and superior
insufficiency of the acetabulum will develop.
Treatment:
- The aim of soft tissue surgery is to restore the normal muscular balance
between agonist and antagonist.
- The restoration of the normal balance would have a greater effect on
the acetabular development if it were performed on younger children under
four or five years of age with appropriate postoperative splinting.
- In the child four years of age and older presenting hip dysplasia may
require a bony procedure for hip stabilization.
*Surgical Indications at A.I. duPont
Children with spasticity secondary to Cerebral Palsy less than eight
years are indicated for tenotomy of the adductor longus and gracilis) if:
- The Reimers Migration Percentage (MP) was greater than 25% and the
hip abduction is 30 degrees or less with hip and knee fully extended, or
- Children with hip abduction 30 to 45 degrees and MP 25 to 50 percent
and demonstrated 10 degree MP increase in one year, or
- MP over 50 with hip abduction less than 45 degrees.
- If less than 45 degrees of hip abduction is present after release of
the adductor longus and gracilis, the myotomy of adductor brevis and anterior
branch obturator neurectomy is performed.
- The tendon of the iliopsoas is completely transected if the patient
is a non ambulator, or the psoas tendon fibers only are cut if an ambulator.
- If the popliteal angle is greater than 45 degrees under anesthesia,
all proximal three hamstrings are transected.
- Distal hamstring lengthening is performed if the popliteal angle is
greater than 45 degrees and the child is already or is predicted to be
a very functional ambulator.
SELECTED LITERATURE REVIEW:
i) ADDUCTORS
-Posterior transfer of hip adductors (add. long., and gracilis) to ischium
(Stephenson and Donovan).---Procedure is more difficult. There is controversy
as to whether this procedure achieves a better functional result than the
simple adductor tenotomy.
-Matsuo reported insufficiency of the hip-adductor after anterior obturator
neurectomy and exaggerated the important role of hip adductors to stabilize
the hip joint.
-The results of adductor tenotomy with or without obturator neurectomy
alone were poor (Samilson,Green,Kalen and Bleck).
ii) ILIOPSOAS
-Bleck recommends the iliopsoas recession ( iliopsoas transfer to the
antero-lateral hip joint capsule) for those who have a subluxation of the
hip joint instead of ilopsoas tenotomy or lengthening by the z-method.
-iii) HAMSTRINGS
-Only a few surgeons exaggerate the necessity of the release of hamstrings
as the treatment for the subluxation of the hip.
-Proximal hamstring lengthening is effective in stabilizing the sitting
posture and preventing the thoraco-lumbar kyphosis in nonambulatory children(
Elmer, Mubarak, Bowen).
REFERENCES:
- Cornell M S: The hip in Cerebral Palsy (Revew Article). Develop. Medicine
and Child Neurol.37: 3-18, 1995.
- Bleck, E E : Orthopaedic Management of Cerebral Palsy, Philadelphia,
J.B. Lippincott Co.,1 987.
- Smith J T, STevens P M: Combined adductor transfer, iliopsoas release,
and proximal hamstring release in cerebral palsy. J. Pediat. Orthop. 9:
1-5,1989.
- Green W T, Mcdermott L J: Operative treatment of cerebral palsy of
spastic type. J.A.M.A. 118: 434-440, 1942.
- Okawa A, Kajiura I, Hiroshima K: Physical therapeutic and surgical
management in spastic diplegia. Clin. Orthop. 253: 38-44,1990.
- Mubarak S J, Francisco G V, Wenger D R. One-stage correction of the
spastic dislocated hip. J Bone and Joint Surg. 74-A: 1347-1356,1992.
- Seymour N, Sharrard WJW: J Bone and Joint Surg. 50-B: 274-277,1968.
- Rang M, Doouglas G, Bennet GC, Koreska J: Seating for children with
cerebral palsy. J Pediat Orthop. 1: 279-287,1981.
- Bowen JR, MacEwen GD, Mathews PA: Treatment of extension contracture
of the hip in cerebral palsy. Develop Med Child Neurl. 23: 23-29,1981.
- Elmer EB, Wenger DR, Mubarak SJ, Sutherland DH: Proximal hamstring
lengthening in the sitting cerebral palsy patient. J Pediat Orthop. 12:
329-336,1992.
- Sharrard WJW, Allen JMH, Heaney SH.Surgical prophylaxis of subluxation
and dislocation of the hip in cerebral palsy. J Bone and Joint Surg. 57-B:
160-166,1975.
- Reimers J: The stability of the hip in children. A radiological study
of the results of muscle surgery in cerebral palsy. Acta Orthop Scand (Suppl.)
.184:1, 1980.
 Hip abduction was 50 degrees and popliteal angle was 10 degrees bilaterally.
In the prone position with her hips extended, she has 60 degrees of internal
rotation bilaterally and 40 degrees of external rotation on the right and
60 degrees of external rotation on the left. She had a negative Thomas
test bilaterally. At 2y.+6m., bilateral iliopsoas release, bilateral
adductor longus and gracilis release were performed. At 4y.+ 2m., she
could ambulate with a walker. Hip abduction was 60 degrees bilaterally.
Popliteal angle was 30 degrees bilaterally, x-ray showed normal hips.
Hip abduction was 50 degrees and popliteal angle was 10 degrees bilaterally.
In the prone position with her hips extended, she has 60 degrees of internal
rotation bilaterally and 40 degrees of external rotation on the right and
60 degrees of external rotation on the left. She had a negative Thomas
test bilaterally. At 2y.+6m., bilateral iliopsoas release, bilateral
adductor longus and gracilis release were performed. At 4y.+ 2m., she
could ambulate with a walker. Hip abduction was 60 degrees bilaterally.
Popliteal angle was 30 degrees bilaterally, x-ray showed normal hips. At 7y.+5m., she underwent bilateral distal hamstring lengthening , rectus
femoris transfer, gastrocnemius recession, and bilateral. lateral column
lengthenings for her crouched gait and valgus foot deformities. Recent
popliteal angles were 25 bilaterally, Thomas test 15 bilaterally, and hip
flexion and abduction were all normal. Six years after adductor lengthening
both hips are normal.
At 7y.+5m., she underwent bilateral distal hamstring lengthening , rectus
femoris transfer, gastrocnemius recession, and bilateral. lateral column
lengthenings for her crouched gait and valgus foot deformities. Recent
popliteal angles were 25 bilaterally, Thomas test 15 bilaterally, and hip
flexion and abduction were all normal. Six years after adductor lengthening
both hips are normal.