SUGIOKA OSTEOTOMY
MASAFUMI HOMMA, M.D.,D.M.Sc, Research Fellow of Orthopaedic Surgery
RICHARD BOWEN, M.D., Pediatric Orthopaedic Surgeon, Chairman
October. 26,1995
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY:
PATIENT 1.
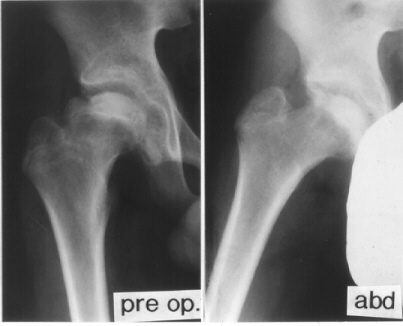
K.B.. 12-year-old boy. B.W. 63 kg(139 Ib.) . Perthes disease.
He had right hip pain and limping for seven weeks. When he was
first seen at University Hospital of Niigata, the right femoral
head was deformed already and collapsed slightly on X-ray. The lateral part of the femoral head showed an impingement lesion.
Because good sphericity of the posterior part of the femoral head
was still preserved,
The lateral part of the femoral head showed an impingement lesion.
Because good sphericity of the posterior part of the femoral head
was still preserved, Sugioka's rotational osteotomy was advised. Pre-operative range
of motion was flex.90, abd.35, e.r. 40, and i.r. 15. The femoral
head was anteriorly rotated by 75 degrees and varus angulation
by 15 degrees was made.
Sugioka's rotational osteotomy was advised. Pre-operative range
of motion was flex.90, abd.35, e.r. 40, and i.r. 15. The femoral
head was anteriorly rotated by 75 degrees and varus angulation
by 15 degrees was made.  Continuous-passive-motion and pulley exercise on a bed was started
from the 1st post-operative day. Skin traction was performed for
2 weeks. After post-operative non-weight-bearing for 4 weeks,
and partial-weight-bearing for 6 weeks, he has had neither limping
nor pain for more than 3 years.
Continuous-passive-motion and pulley exercise on a bed was started
from the 1st post-operative day. Skin traction was performed for
2 weeks. After post-operative non-weight-bearing for 4 weeks,
and partial-weight-bearing for 6 weeks, he has had neither limping
nor pain for more than 3 years.
PATIENT 2.
W.H.. 12-year-old-girl. Post-traumatic avascular necrosis of rt.
femoral head. She sustained the right femoral neck fracture by
falling from a balcony. After bed-rest for 2 weeks, she started walking with crutches.
She completely returned to normal activities 6 months after the
trauma. She was beginning to complain of the right hip pain 2
years after the trauma. A large area of avascular necrosis was
in weight bearing surface of the femoral head.
After bed-rest for 2 weeks, she started walking with crutches.
She completely returned to normal activities 6 months after the
trauma. She was beginning to complain of the right hip pain 2
years after the trauma. A large area of avascular necrosis was
in weight bearing surface of the femoral head.
 The large posterior surface of the femoral head remained intact.
A Sugioka osteotomy was performed with 90 degrees of anterior
rotation and 15 degrees of varus angulation. After post-operative
non-weight-bearing for 4 weeks, and partial-weight-bearing for
6 weeks, she has had neither limping nor pain so far.
The large posterior surface of the femoral head remained intact.
A Sugioka osteotomy was performed with 90 degrees of anterior
rotation and 15 degrees of varus angulation. After post-operative
non-weight-bearing for 4 weeks, and partial-weight-bearing for
6 weeks, she has had neither limping nor pain so far.
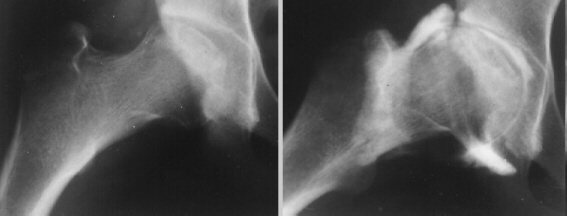
PREOPERATIVE PLANNING:
- Anteroposterior and true lateral radiographs should be performed.
For the true lateral radiograph, the patient should be positioned
supine, with the hip in precisely 90 degrees of flexion and 45
degrees of abduction and with neutral rotation.
- The preoperative lateral view radiograph shows the A-P view
of the femoral head as it will appear after 90 degrees of posterior
rotation.
- In contrast, a preoperative lateral view in a reversed position
shows the A-P view after 90 degrees of anterior rotation.
OPERATIVE PROCEDURE:
- Skin incision: a modified Ollier's incision, or a lateral
oblique incision.
- Osteotomized the greater trochanter and reflect it proximally
with the gluteus medius muscle.
- Transect the short external rotator muscles and quadratus
femoris muscle. Care must be taken to avoid injury to the posterior
branch of the medial circumflex artery, which lies just above
the lesser trochanter and can easily be seen at the time of transection
of the short rotators and the quadratus femoris muscle.
- A circumferential incision is made in the hip joint capsule
near the acetabular rim.
- The first osteotomy is made, 10mm distal to the intertrochanteric
crest, toward the lesser trochanter, and in a plane perpendicular
to the neck in every direction.
- To determine the osteotomy plane, two K-wires are placed through
the denuded surface of the greater trochanter both anterioly and
posterioly in a plane perpendicular to the another K-wire which
is placed along the femoral neck.
- A second osteotomy is performed from the upper margin of the
lesser trochanter to the first osteotomy line.
- When an anterior rotation of 70 degrees or more is required,
the iliopsoas tendon should be transected near the lesser trochanter
before rotation.
- Two large pins are inserted parallel into proximal and distal
fragments, and femoral head is rotated anteriorly by handling
proximal pin.
- After adequate rotation, a large screw is inserted in valgus
position. An A-P X-ray should be taken to ensure the weight-bearing
portion is well apposed and the neck-shaft angle. Then a Steinman
pin is removed and another large pin is inserted. The A-O compression
screw is ineffective because of its thin shank.
- The intentional varus position may be made in addition to
anterior rotation for an extensive lesion.
POSTOPERATIVE MANAGEMENT
- Two kg of skin traction all day for 1 week and at night for
additional 2 weeks.
- Quadriceps setting and active ROM exercise should be started
within 10 days.
- Walking exercise in a pool is usually allowed 5 to 6 weeks
after surgery.
- Partial weight bearing is started at 8 weeks and continued
for 6 months after surgery.
COMPLICATIONS:
- Early: Fracture of lessor trochanter, Subtrochanteric fracture
- Late: Deep infection, Neck fracture, Delayed union, Nonunion
of greater trochanter,
CLINICAL RESULTS:
- Sugioka classifed the preoperative hips into four grades:
grade 1, necrosis just visible, the femoral head is still round;
grade 2, the head is flattened; grade 3, the head is markedly
collapsed without narrowing of the joint space; and grade 4, the
head shows advanced changes with narrowing of the joint space.
- The success rate in the 23 hips of grade1 was 91%, in the
16 hips of grade 2 was 88%, in the 64 hips of grade3 was 73%,
and in the 25 hips of grade 4 was 68%.
- Seventy-six of the 80 hips in which the intact area on the
preoperative lateral view was more than one third of total joint
surface showed no collapse of the newly created weight-bearing
area (success rate: 95%). On the other hand, twenty-one of 48
hips in which the intact area was less than one third showed progressive
collapse (success rate: 56%).
- Only three of 85 hips in which the intact area on the post-operative
A-P view was greater than 36% showed further collapse (success
rate: 96%). But five of the 22 hips in which the intact area was
ranged from 21-31%, and 17 of the 21 hips in which the intact
area was less than 20% showed further collapse (success rate:
77%, and19% respectively).
INDICATIONS:
- Idiopathic, steroid-induced, post-traumatic and other symptomatic
osteonecrosis of the femoral head, Perthes' disease, slipped capital
femoral epiphysis, primary osteoarthritis with localized erosion
in the weight-bearing area, are indications for application of
this procedure.
- Contraindications: 1, total necrosis; 2, complication with
poor prognosis (obesity etc.)
- Indications: 1, Sugioka's grade I or II lesion; 2, grade III
or IV lesion in which extent of lesion is under two thirds in
lateral x-ray view; 3, unilateral grade III or IV lesion in which
extent of lesion is over two thirds.
- Relative indications: 1, Bilateral grade III or IV lesion
in which extent of lesion is over two thirds in younger patient.
REFERENCES:
- Sugioka Y.: Transtrchanteric rotational osteotomy of the femoral
head. In Riley, L.H.Jr.(ed.): The Hip. Proceedings of the Eighth
Open Scinentific Meetingof the Hip Society. St. Louis, C.V. Mosby,
1980.pp.3-23.
- Sugioka Y.: Transtrochanteric anterior rotational osteotomy
of the femoral head in the treatment of osteonecrosis affecting
the hip: A new osteotomy operation. Clin. Orthop. 130: 191-201,1978.
- Sugioka Y., Katsuki I., and Hotokebuchi T.: Transtrochanteric
rotational osteotomy of the femoral head for the treatment of
osteonecrosis: Follow-up statistics. Clin. Orthop. 169: 115-126,1982.
- Sugioka Y.: Transtrochanteric rotational osteotomy in the
treatment of idiopathic and steroid-induced femoral head necrosis,
Perthes' disease, slipped capital femoral epiphysis, and osteoarthritis
of the hip: indications and results, Clin. Orthop. 184: 12-23,1983.
 The lateral part of the femoral head showed an impingement lesion.
Because good sphericity of the posterior part of the femoral head
was still preserved,
The lateral part of the femoral head showed an impingement lesion.
Because good sphericity of the posterior part of the femoral head
was still preserved, Sugioka's rotational osteotomy was advised. Pre-operative range
of motion was flex.90, abd.35, e.r. 40, and i.r. 15. The femoral
head was anteriorly rotated by 75 degrees and varus angulation
by 15 degrees was made.
Sugioka's rotational osteotomy was advised. Pre-operative range
of motion was flex.90, abd.35, e.r. 40, and i.r. 15. The femoral
head was anteriorly rotated by 75 degrees and varus angulation
by 15 degrees was made.  Continuous-passive-motion and pulley exercise on a bed was started
from the 1st post-operative day. Skin traction was performed for
2 weeks. After post-operative non-weight-bearing for 4 weeks,
and partial-weight-bearing for 6 weeks, he has had neither limping
nor pain for more than 3 years.
Continuous-passive-motion and pulley exercise on a bed was started
from the 1st post-operative day. Skin traction was performed for
2 weeks. After post-operative non-weight-bearing for 4 weeks,
and partial-weight-bearing for 6 weeks, he has had neither limping
nor pain for more than 3 years.