OSTEOGENESIS IMPERFECTA OR NON-ACCIDENTAL
INJURY:
HOW CAN YOU TELL?
Richard W. Kruse, D.O.,H. Theodore Harcke, M.D., Caitlin Minch,
Milan Moore, M.D.
Alfred I. duPont Institute, Wilmington, Delaware USA
Key Points of This Exhibit
- The diagnosis of OI is primarily based on meticulous history and
physical examination.
- Skin biopsy remains the most sensitive test. It may require three
months for results to be available.
- It is possible to have OI and a normal skin biopsy.
- Bone densitometry (DEXA) is a useful adjunct in the rapid determination
of low bone density as a risk factor for fracture.
INTRODUCTION
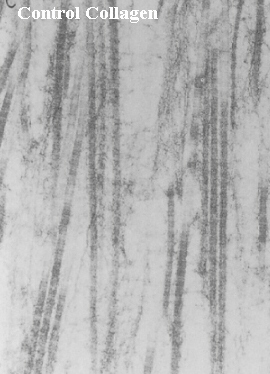
Osteogenesis imperfecta (OI) is a rare generalized connective tissue
disorder arising from defects in the structure and/or function of type
I collagen. Although there is a great deal of phenotypic variability in
this disorder, most patients have osseous fragility that results in frequent
fractures. The milder clinical forms may be difficult to diagnose and may
be confused with non-accidental injury (NAI). We present differential diagnostic
points that aid the clinician. We also sought to examine the emerging role
of dual-energy x-ray absorptiometry (DEXA) in the evaluation of the patient
with multiple fractures. This review should not be considered as a definitive
or complete differential diagnosis of frequent fractures, but is meant
to present certain clinical points that may be of assistance to the clinician.
A team approach with input from pediatrician, orthopaedist, geneticist,
radiologist, social work, and legal services is recommended when dealing
with potential non-accidental injury.
Dual-Energy X-ray Absorptiometry (DEXA)
- We conducted a study to assess the role of DEXA in the workup of the
pediatric patient with multiple fractures. A retrospective study identified
33 patients presenting to the A.I. duPont Institute with multiple fractures
who had DEXA scan as part of their workup. Twenty-seven had sufficient
clinical data to make a diagnosis of OI. Patients underwent DEXA of the
anteroposterior spine, pelvis, and whole body when technically feasible.
DEXA values were normalized for age using published standards developed
at our institution. We correlated the diagnosis of OI to outcome of each
DEXA scan to determine the sensitivity and specificity.
- DEXA of the anteroposterior spine had the highest sensitivity at
90.9% while DEXA of the whole body
 had the highest specificity at 81.3%. These were highly statistically significant.
DEXA of the pelvis and DEXA not normalized for age were less predictive.
Age adjusted scores for all body regions tested were 78% to 85% accurate
in this population.
had the highest specificity at 81.3%. These were highly statistically significant.
DEXA of the pelvis and DEXA not normalized for age were less predictive.
Age adjusted scores for all body regions tested were 78% to 85% accurate
in this population.
- Despite this, 1/11 patients with OI had normal DEXA values while 4/16
patients without OI had low DEXA.
- DEXA has a role in the evaluation and quantitation of osteopenia as
a risk factor for fracture. Skin biopsy remains the most definitive at
this time, but is not I 000/o sensitive.
Non-accidental Injury
Suspicious History
- fracture in absence of significant trauma
- history inconsistent with fracture pattern or timing
- delay in reporting
- lack of repeated fractures in protected environment
- visceral or unusual skin injuries
- head or cerebral injury
X-ray Fracture Patterns
- none pathognomic
- bucket handle or metaphyseal corner (virtually pathognomic)

- multiple fractures in different healing stage
- posterior rib near costovertebral junction (virtually pathognomic)

- lower extremity in non-weight bearing child
- acute epiphyseal in very young child
- acute bilateral extremity
Osteogenesis imperfecta
History/Physical
- frequent fractures, minimal trauma
- blue sclerae
- easy bruisability
- joint laxity
- discolored or softened teeth (dentinogenesis imperfecta)
- short stature
- abnormal skull shape
- heat intolerance or excessive sweating
- family history of above features
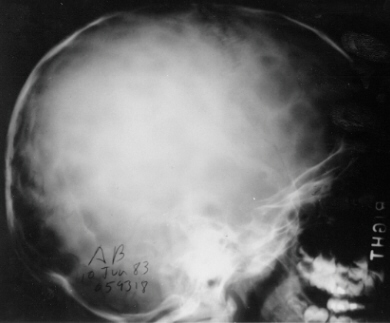
X-ray/Diagnostic Imaging
- bone deformity or osteopenia
- wormian bones

- sutural bones 6 mm x 4 mm or larger, often more than 10 mm in number,
in a mosaic pattern
- absent in normal skulls
- indicator of abnormal bone condition (extensive differential diagnosis)
- found in almost all patients with OI except some neonates in which
the skull is insufficiently ossified, and in adults with technically poor
x-ray
Skin Biopsy
- 2-3 mm in standard tissue culture medium
- sent to cell culture facility
- abnormal structure or synthesis of type I Collagen identifiable in
approximately 85%-90% of patients with OI


- in one study of OI vs NAI most OI was suspected clinically
prior to biopsy
Byers PH - personal communication 3 Aug 1994.. Studied 53 samples
submitted to their laboratory for Collagen screening to evaluate OI vs
NAI. 6/53 had biochemical evidence of OI. Review of the clinical features
of OI on clinical exam, usually blue sclerae or osteoporosis, bone deformity,
or short stature. The referring physician suspected OI in 4/6 after physical
exam. Radiographic features including type of fracture were nonspecific.
In the remaining 47 patients, no fractures were noted in protecfive custody.
Differential Diagnosis In OI
AGE DIFFERENTIAL DIAGNOSIS
Prenatal - Thanotophoric Dysplasia
- Autosomal Recessive Hypophosphatasia
- Achondrogenesis
- Campomelic Dysplasia
Newborn/Early Childhood - Campomelic Dysplasia
- Non-accidental Injury
- Hypophosphatasia
- Cystinosis
- Leukemia
- Achondroplasia
Childhood/Adolescence - Non-accidental Injury
- Juvenile Osteoporosis
- Osteoporosis
- Pyknodysostosis
- Leukemia
References:
- Ablin DS, Greenspan A, Reinhart M, Grix A. Differentiation of Child
abuse from osteogenesis imperfecta. Zionts I P, Nash JP,
Rude R, Ross T, Staff NS. Bone mineral density in children with mild osteogenesis
imperfecta. J Bone Joint Surg 1995;77B: 143-147.
- Davie MW, Haddaway MJ. Bone mineral content and density in healthy
subjects and in osteogenesis imperfecta. Arch Dis Child 1994;70:331-334.
- Ablin DS, Greenspan A, Reinhart M, Grix A. Differentiation of child
abuse from osteogenesis imperfecta. AJR 1990; 1 54:1035-1046.
- Kleinman PK, Marks SC, Blackbourne B. The metaphyseal lesion in abused
infants: a radiologic-histopathologic study. AJR 1986; 1 46:895-905.
- Wenstrup FJ, Willing MC, Starman BJ, Byers PH. Distinct biochemical
phenotypes predict clinical severity In non-lethal variants at osteogenesis
imperfecta. Am J Hum Genet 1990;46:975-982.
- Harcke HT. imaging of the immature skeleton. In Lovell and Winter's
Pediatric Orthopaedics, vol. 1, (3rd ed.), RT Morrissy, ed, Philadelphia:
JB Lippincott, 1990.
- Taylor A. Norman ME, Konard P, Harcke HT, Whole body bone mineral
density: normative values for children 2-9 years of age, J Bone
Mineral Res 1994,9:S292.
Orthopaedic Department Home Page, Radiology
Department Home Page, Osteogenesis Imperfecta
Home Page, Top (DEXA Exhibit)