AN EARLY SIGN OF AVASCULAR NECROSIS AND LATE LATERAL
GROWTH ARREST OF THE PROXIMAL FEMUR IN DEVELOPMENTAL DISLOCATION OF THE
HIP
MASAFUMI HOMMA, M.D., D.M.Sc, Research Fellow of Orthopaedic Surgery
JAY KUMAR, M.D., Pediatric Orthopaedic Surgeon
March 13, 1996
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY:
A ten year old female presented with a left hip dislocation. She was
born by Cesarean-section because of slow progression of labor. The child
was not breech and was noted to have a dislocatable hip at birth. There
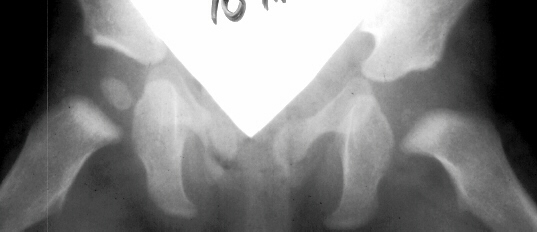
was a negative family history of DDH. An X-ray prior to application of
the brace showed the dislocation of the hip. The patient was first seen
at AIDI on 9th day. Abduction of the right hip was 80 degrees but left
was only 60 degrees. There was a positive Galeazzi sign with the left hip
being shorter than the right. X-rays showed a left hip dislocation and
right hip subluxation  .
A Pavlik harness was applied. After two months, the right hip improved
but the left hip was still dislocatable
.
A Pavlik harness was applied. After two months, the right hip improved
but the left hip was still dislocatable .
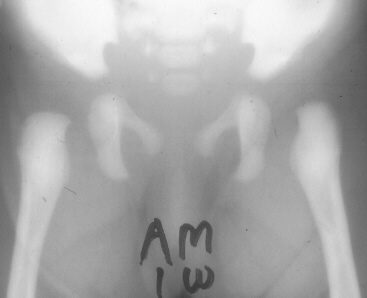
For this, home traction was started. Even after 2 months, the left hip
did not reduce
.
For this, home traction was started. Even after 2 months, the left hip
did not reduce .
Therefore, an arthrogram, adductor tenotomy and closed reduction was done
at 4 months of age
.
Therefore, an arthrogram, adductor tenotomy and closed reduction was done
at 4 months of age .
Single hip spica was applied with the hip in 40 abduction and 100 flexion.
Eight weeks later an arthrogram was performed
.
Single hip spica was applied with the hip in 40 abduction and 100 flexion.
Eight weeks later an arthrogram was performed  and the cast was reapplied with the hip in 35 degrees abduction and 100
degrees flexion.
and the cast was reapplied with the hip in 35 degrees abduction and 100
degrees flexion.
Four months later, the spica cast was removed and an Atlanta brace was
applied. X-rays showed avascular necrosis at ten months of age  .
At two years of age, the ossification of the left nucleus was still delayed.
The leg lengths were equal and the range of motion of the hip was full.
.
At two years of age, the ossification of the left nucleus was still delayed.
The leg lengths were equal and the range of motion of the hip was full.
The progression of the hip is documented by x-rays taken at 1 year of
age ,
2 years of age
,
2 years of age ,
3 years of
,
3 years of
age ,
5 years of age
,
5 years of age ,
7 years of age
,
7 years of age ,
then at ten years of age
,
then at ten years of age ,
early closure of the lateral portion of proximal growth plate observed.
Coxa valga was also observed.
,
early closure of the lateral portion of proximal growth plate observed.
Coxa valga was also observed.
Incidence of avascular necrosis of the femoral head in DDH:
- The reported incidence of avascular necrosis has ranged from zero to
73 per cent.
Factors related to avascular necrosis in DDH:
- Most authors agree that the etiology is vascular in origin.
- Variation in the mode of treatment has resulted in a decrease in the
incidence of this complication: early diagnosis; preoperative traction;
gentle reduction with the use of general anesthesia; adductor tenotomy;
avoidance of an extreme abducted position of immobilization.
- Age: a non-ossified femoral head (birth to six months) is more susceptible
to damage to the blood supply than an ossified femoral head (after the
age of six month).
- Boys are more susceptible to ischemia than girls.
The importance of growth plate involvement:
- Ischemic necrosis may affect the ossific nucleus with or without involvement
of the proximal growth plate. The subtle signs of physeal involvement were
far less obvious than the changes in the ossific nucleus. But it plays
a key role in the future development of femoral head deformities.
Kalamchi and MacEwen's classification of avascular necrosis in DDH(1980):
- Group I. Changes Affecting the Ossific Nucleus
Either delay in the appearance of the ossific nucleus or mottling of
the ossific nucleus. With revascularization, there is flattening and fragmentation
of the shadow of the ossific nucleus, but the head will usually regain
its spherical shape. Some femoral heads will show the head-within-head
appearance. This is the most common with the best prognosis.
- Group II. Lateral Physeal Damage
The initial changes in the ossific center may follow exactly those seen
in Group I, but in addition there is damage to the lateral part of the
physis. The early roentgenographic signs indicating lateral physeal damage
are: (1) lateral ossification, (2) lateral physeal irregularity and bridging,
(3) lateral notching of the epiphysis, and (4) a lateral metaphyseal defect.
The damage to the physis may remain dormant. By the age of ten years,
however, valgus deformity of the head on the neck develops.( This type
occurred in 35% of total AVN at AIDI.)
- Group III. Central Physeal Damage
The early changes in the ossific nucleus are similar to those observed
in Group I and II. The damage to the growth plate is more centrally located.
Commonly, patients develop a short femoral neck without varus or valgus.
Relative overgrowth of the greater trochanter and limb length discrepancy
are the principal problems.
- Group IV. Total Damage to the Head and the Physis
Damage of the entire femoral head and physis are characteristic of this
group. Early irregular femoral head with varus, flattening, and coxa magna.
Overgrowth of the greater trochanter, limb length discrepancy, and subsequent
early arthritis are the principal complications.
Bucholz and Ogden's classification (1978):
- Type I. Complete fragmentation of the capital femoral ossific nucleus.
Physis shows no irregularities and no propensity to premature closure.
Minimal to mild residual deformity.
- Type II. The physis became irregular in its lateral aspect soon after
fragmentation of the ossification center. Localized premature fusion of
the superolateral portion of the plate. This premature fusion is not evident
until the patients are 7 to 12 & half years of age, with the
mean age of roentgenographically evident partial premature fusion being
9 years.
- Type III. The entire physis is irregular, and premature fusion of the
entire plate occurred at an average age of 7 and half years. Marked coxa
vara with a variably deformed femoral head, an extremely short femoral
neck, and severe overgrowth of the greater trochanter.
- Type IV. Variable abnormalities that seem to affect the medial epiphyseal
ossification center and to a lesser degree, the medial metaphysis. Severe
coxa magna with shortening of the femoral neck.
Treatment
- Kalamchi type I: Observation / Bracing.
- Kalamchi type II: Observation / Varus osteotomy &/or proximal epiphysiodesis.
- Kalamchi type III/IV: Apophyseodesis or distal trochanteric transfer
for trochanteric overgrowth. Shoe lift or properly-timed epiphysiodesis
for limb length inequality.
References:
- Borges JL, Jayakumar S, Guille JT: Congenital dislocation of the hip
in boys. J Bone and Joint Surg.77-A: 975-983, 1995.
- Kalamchi A, McEwen GD: Avascular necrosis following treatment of congenital
dislocation of the hip. J Bone and Joint Surg. 62-A: 876-887,1980.
- Bucholz RW, and Ogden JA: Patterns of ischemic necrosis of the proximal
femur -Nonoperatively treated congenital hip disease. In The Hip: Proceedings
of the Sixth Open Scientific Meeting of the Hip Society, pp. 43-63. St.
Louis, C.V. Mosby,1978.
- Kasser KR, Bowen JR, MacEwen D:Varus Derotation Osteotomy in the treatment
of persistent dysplasia in congenital dislocation of the hip. J Bone and
Joint Surg. 47-A: 195-202, 1985.
- Thomas IH, Dunin AJ, Cole WG, Menelaus MB: Avascular necrosis after
open reduction for congenital dislocation of the hip: Analysis of causative
factors and natural history. J Pediat Orthop. 9: 525-531,1989.
- O'Brien MC, Millis MB, Griffin PP: The early identification and classification
of growth disturbances of the proximal end of the femur. J Bone and Joint
Surg. 68-A: 970-980,1986.
- Jones DA: Sub-capital coxa valga after varus osteotomy for congenital
dislocation of the hip: A report of six cases with a minimum follow-up
of nine years. J Bone Joint Surg. 59-B:152-158,1977.
 .
A Pavlik harness was applied. After two months, the right hip improved
but the left hip was still dislocatable
.
A Pavlik harness was applied. After two months, the right hip improved
but the left hip was still dislocatable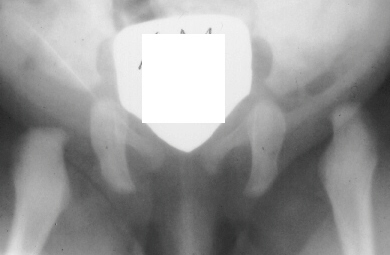 .
For this, home traction was started. Even after 2 months, the left hip
did not reduce
.
For this, home traction was started. Even after 2 months, the left hip
did not reduce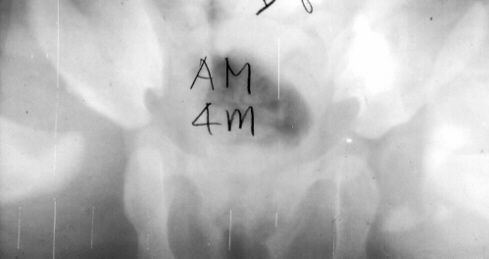 .
Single hip spica was applied with the hip in 40 abduction and 100 flexion.
Eight weeks later an arthrogram was performed
.
Single hip spica was applied with the hip in 40 abduction and 100 flexion.
Eight weeks later an arthrogram was performed 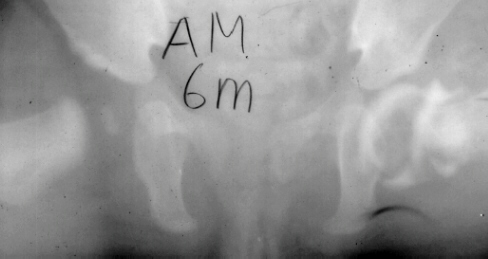 and the cast was reapplied with the hip in 35 degrees abduction and 100
degrees flexion.
and the cast was reapplied with the hip in 35 degrees abduction and 100
degrees flexion.