OSTEOCHONDROMA (Multiple Exostosis)
Frank Cuce, D,O., Resident Orthopaedic Surgery
KIRK W. DABNEY, M.D,, Attending Orthopaedic Surgery
June 19, 1996
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY:
HISTORY
S.G. is a 12 year old BF who presented with a chief complaint of left
knee pain on the medial aspect of the proximal tibia. The pain was described
as a dull, aching pain present for one year's time, occassionally awakening
her from sleep and occassionally worsening with sports activities.
Her past medical history was essentially unremarkable. There was a questionable
family history for "bony tumors".
PHYSICAL EXAMINATION
Physical examination revealed full range of motion of all her extremities.
She was neurovascularly intact. DTR's were normal and symmetric. Palpation
at the left knee revealed an asymptomatic mass at the distal femur medially
and a painful protrusion at the medial proximal tibia.
XRAYS
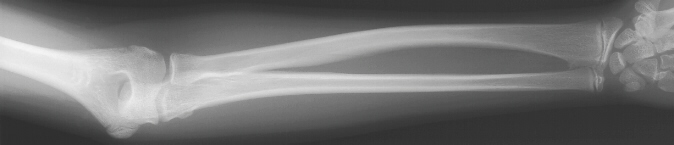
X-rays of her left knee in the AP/lat/oblique views revealed multiple
exostoses of the distal femur and proximal tibia. These were also noted
in bilateral forearm films at the proximal and distal poles 

 .
.
DISPOSITION OF CASE
Secondary to the painful nature of the proximal tibial osteochondroma,
it
was excised. She was placed in a knee immobilizer and discharged on
POD #1.
DISCUSSION
- Most common benign bone tumor
- 90% solitary lesions
- Sessile/pedunculated
- Bone covered by cartilage cap up to 3cm thick
- 10% occur in the heritable form of multiple exostosis
- Male/female(1:1), 80% diagnosed in first decade of life
- Malignant transformation reported up to 20%
- As reported by Shapiro et al. associated with ulnar deformation, radialhead
dislocation, and rotation limitations in the upper extremity; coxa valga,
genu valgum, genu recurvatum, obliquity of distal tibial physis and LLD
in the lower extremities
ETIOLOGY
Two theories:
- Virchow in 1891 - Physeal theory where portion of plate separates and
rotates 90 degrees; he could not substantiate.
- Plate defect theory proposed by Keith in 1920 and supported by studies
done by D'Ambrosia and Ferguson in 1968. They produced exostoses by physeal
cartilage transplantation demonstrating and supporting the concept that
exostoses are developmental physeal growth defects.
GROWTH
- Occurs by enchondral ossification of the cartilage cap mimicking physeal
growth
- Traditional teaching states growth parallels that of parent physis
- However, Lange et al, in 1984 demonstrated activity of exostoses well
beyond skeletal maturity via bone scan
INDICATIONS FOR EXCISION
- Development of painful bursae
- Location that subjects tumor to recurrent injury
- Significant cosmetic deformity
- Clinical or radiographic suspicion that malignant degeneration has
occurred
- Cardelia et al. 1995, reported six cases of peroneal nerve palsy associated
with proximal fibular osteochondroma
COMPLICATIONS
- Malignant degeneration is most significant of potential problems
- Risk for malignant change is cited as approximately 1% for solitary
and 20% for patients with multiple lesions
- Frequent sites include proximdl femur/humerus for solitary lesions
and pelvis/scapuld for multiple hereditary exostoses
- Malignant change evolves slowly; usually occurs in adulthood and is
associated with recent onset of pain
- Average age is 30.7 years as reported by Garrison
- Lange et al. in 1984, correlated the x-ray, bone scan and histologic
findings in 24 patients with solitary or multiple exostoses and found malignant
degeneration is 2 of 25 exostoses.
- Both exostoses were found in an "active" pattern by bone
scan
- The bone scan could not however, differentiate benign active exostoses
and chondrosarcoma
- Prognosis after excision is excellent
- Pseudoaneurysm
- Rare complication of exostosis of the femur
- No true layers (intima/media/advantitia)
- Only intimal layer in fibrous capsule
- Caused by repeated injury to artery
- i.e. repeated puncture from bone spikes after fracture
- gradual erosion by repeated activity i.e. bicycling
REFERENCES:
- Lange RH, et al. Correlative Radiographic, Scintigraphic, and Histologic
Evaluation of Exostoses. JBJS 66A;9:1454-1459 1984.
- Cardelia JM, et al. Proximal Fibular Osteochondroma with Associated
Peroneal Nerve Palsy: A review of six Cases. JPO 15:574-577, 1995.
- Shapiro F, et al. Hereditary Multiple Exostoses. JBJS 61A;6:815-824,
1979.
- Solomon L. Hereditary Multiple Exostosis, JBJS, 45B;2:292-3049 1963.
- D'Ambrosia R, Ferguson ABR. The Formation of Osteochondroma by Epiphyseal
Cartilage Transplantation. Clin, Orthop, 61:103, 1968.
- Enneking WF. Musculoskeletal Tumor Surgery. Surgical Considerations
in Specific Tumors. ed. Churchill Livingstone Inc., New York, Vol
21 892-913@ 1983.
 .
.