SKEWFOOT IN CHILD WITH UNDIAGNOSED SKELETAL DYSPLASIA
Scott Norris, D.O., Orthopaedic Resident
Dan Mason , M.D., Attending Pediatric Orthopaedic Surgeon
Sept. 19, 1995
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY:
This is a 6 year old white male, with an undiagnosed skeletal dysplasia,
who has been followed for 5.5 yrs. Previous surgery includes bilateral
femoral and tibial osteotomies for bilateral valgus deformities with good
results. His foot deformity has never been treated with with casts or splints,
but has worn AFO braces for persistent valgus hind foot deformities. Present
exam reveals the following bilateral foot deformities.
- hindfoot valgus of approx. 20-30 degrees
- metatarsus adductus
- prominence of the talar head in the medial arch with thickened callus
over the bony prominence
Radiographs reveal the following deformities:
- hindfoot valgus with AP talocalcaneal angle of > 35 degrees



- lateral subluxation/dislocation of the navicular from the talar head
- adduction of the metatarsals with the talus- 1st metatarsal angle to
be divergent medially
- increased lateral talocalcaneal angle with talus plantarflexed on calcaneus


Due to persistent foot pain and excessive callus formation over the
medial arch the patient was taken to the OR and underwent surgical treatment
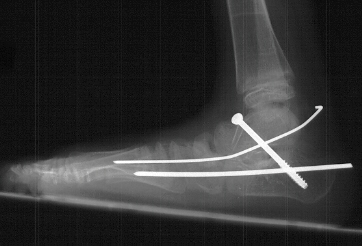
of the left foot. The procedure consisted of :
- subtalar arthrodesis with autograft bone graft and screw fixation


- closing wedge calcaneocuboid arthrodesis with open pinning
- reduction and open pinning of the talonavicular joint
- midfoot soft tissue release of the talonavicular, calcaneocuboid and
subtalar joints
Post operatively, the patient was placed in a long leg cast. Preliminary
results show satisfactory reduction of the talonavicular joint, correction
of hindfoot valgus, dorsiflexion of the talus on the calcaneus, and correction
of forefoot adduction immediately post op.

REVIEW OF SKEWFOOT DEFORMITY:
Definition - also known as serpentine foot, Z foot , Zed foot
-foot deformity consisting of forefoot adduction and plantarflexion,
hindfoot valgus, and
lateral displacement of the midfoot characterized by lateral displacement
of the navicular
on the talar head
GENERAL FEATURES:
- deformity lies along the continuum of metatarsus adductus and hindfoot
valgus
- incidence is rare but may be more common then reported if milder forms
are included,as there are no absolute criteria for the diagnosis of skewfoot
- resistant metatarsus adductus may be a presentation of skewfoot
CLINICAL FEATURES:
- most obvious features are forefoot adduction and hindfoot valgus
- prominence of the talar head in the medial arch with possible flattening
of the medial arch and presence of thickened callus over the head of the
plantarflexed talus
- tendoachilles contracture of variable degree
- deformity may be rigid or supple
RADIOGRAPHIC FEATURES:
- lateral displacement of the navicular on the head of the talus
-navicular ossification however does not occur until 1-2 yrs in females
and yrs in males
- metatarsal adduction
- line drawn through the long axis of the first metatarsal and line drawn
through the long axis of the talus should be parallel or divergent laterally
in the normal foot on AP radiograph
- widening of the talocalcaneal angle on AP radiograph- usually greater
than 35 degrees
- increased lateral talocalcaneal angle with planterflexion of the talus
TREATMENT:
NONOPERATIVE TREATMENT
- serial casting is the mainstay of nonoperative care: application of
the cast is similar to that for metatarsus adductus, but the heel is held
in neutral to slight varus
- successful nonoperative treatment would constitute improvement of foot
appearance, reasonable correction of radiographic features
- cast treatment for skewfoot is longer duration than that needed for
metatarsus adductus
- usual serial casting for approximately 8-10 weeks and 2-4 weeks of
static casting
OPERATIVE TREATMENT
usually not indicated until early childhood, but there are no studies
which delineate the optimal time for surgery
PROBLEMS TO ADDRESS WITH SURGICAL CORRECTION:
- forefoot adduction
- deformity of the medial cuneiform tissue contracture-Achilles, toe
flexors, tibialis posterior, plantar fascia
- lateral displacement of the navicular
- lateral displacement and valgus of the calcaneus
- increased lateral column length
-all of this deformities are variable in severity
Coleman recommends: opening wedge osteotomy of the medial cuneiform,plantar
fascia release, and possible lateral column lengthening (1)
Kendrick and Herndon: subtalar fusion or triple arthrodesis with forefoot
correction (2)
Mosca: lateral calcaneal lengthening with trapezoidal graft, plantarmedial
opening of the medial cuneiform to correct forefoot adduction (3)
GENERAL CONSIDERATIONS FOR OPERATIVE TREATMENT (4)
- younger children consideration should be given to soft tissue releases
and limited bony procedures particularly if the foot is flexible
- older children should consideration should be given to the procedures
above and possible oblique calcaneal osteotomy to correct hindfoot valgus
- adolescents- triple arthrodesis combined with multiple metatarsal osteotomies
and soft tissue releases
CONCLUSIONS ON OPERATIVE TREATMENT:
- skewfoot is a complex deformity and no one procedure can address the
spectrum of deformities nor can one procedure be applied to all age groups
- operative treatment therefore should be planned according to the physical
exam in combination with the known radiographic abnormalities.
REFERENCES:
- Coleman SS. Complex Foot Deformities in Children Philadelphia: Lea
& Fibiger, 1983:267
- Kendrick RE, Sharma NK, Hassler WL, Herndon CH., Tarsometatarsal Mobilization
for Resistant Adduction of the Forepart of the Foot. JBJS (AM) 1970;52:61
- Mosca V. Calcaneal Lengthening for Valgus Deformity of the Hindfoot,
JBJS (AM) Vol. 77-A, No 4:500
- Lovell and Winter's Pediatric Orthopaedics- 3rd ed., Vol. 2 Philadelphia
p.998-1001
- Berg E., A Reappraisal of Metatarsus Adductus and Skewfoot JBJS (AM)
Vol. 68-A, No 8:1185