SOFT TISSUE HEMANGIOMA
MAGDY M ABDEL-MOTA'AL M.D., Orthopaedic. Research Fellow.
ROBERT P STANTON M.D., Attending Pediatric Orthopaedic Surgeon
April 11, 1996
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY:
AM is a 6 year old female who presented to Outpatient Clinic with mass
in her left foot.
PAST MIDICAL HISTORY
On 6-2-95: Excision biopsy of mass of the left foot. Intra-operative
finding revealed a fatty vascular tumor at the planter aspect of the medial
left foot which was infiltrative and adherent to the medial plantar artery
the medial planter nerve, the flexor hallucis longus as well as the flexor
tendon of the second, third, and fourth toes. The pathology report was
a benign lesion.
On 11-7-95: Lower extremity arteriogram with transcatheter embolisation
of left foot arteriovenous malformation.
PHYSICAL EXAMINATION:
There was firm tender mass within the planter arch area of the left
foot. the mass was approximately 6.5 x l7 cm. It involved virtually
the entire arch of the foot. there was a well healed scar that runs longitudinally
over the medial arch portion of the foot.
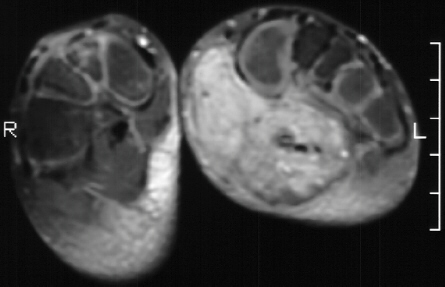
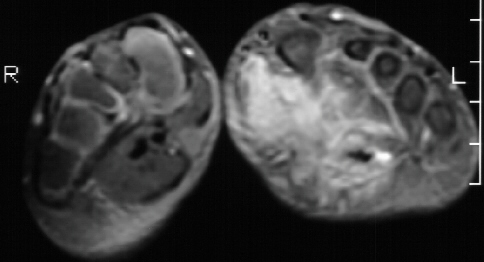
MRI
Suggestive of a vascular hemangioma. 
TREATMENT:
Mass excision. The abductor hallucis muscle was fibrosed. There was
a vascular mass deep and lateral to the abductor hallucis muscle. The mass
and the muscle were excised after careful dissection of the medial plantar
nerve.
DISCUSSION: HEMANGIOMA
These benign vascular processes has been variously thought to
represent hamartomatous malformations of normal vascular tissues or to
represent benign neoplasm.
Age: They arise in childhood and adolescence, and although they persist
indefinitely, they rarely first become apparent in later adult life.
Site: They are most common in the skin and subcutaneous tissues, appear
often in the deep fascia and muscle and are exceptionally rare in bone.
Clinical presentation:
- The superficial lesions presents as a painless mass that has a distinctive
bluish tinge. They are soft and easily compressed.
- The deep lesions present because of intermittent but persistent discomfort
They seldom have any physical signs.
Histology:
- The capillary form is composed of masses of capillaries, communicates
freely with the systemic circulation and may be quite red in appearance.
- Cavernous hemangiomas are composed of large, dilated, tortuous, thin
walled endothelial cavities that when lying superficially, appear blue
in color. They have little anastomosis with the systemic circulation. They
intermittently increase and decrease in size, and have episodes of significant
tenderness associated with episodes of clotting.
Staging Studies:
- X-ray:
- Capillary hemangiomas seldom show even a discernible soft tissue mass.
- Cavernous hemangiomas are frequently visible because of areas of calcification
within them. These calcification are phleboliths caused by clotting in
the cavernous cavities.
- Isotope scans:
- Capillary hemangiomas may show a modest increase consistent with the
increased blood supply, but scans are seldom indicated for surgical planning.
- Angiograghy:
- Angiograghy readily and accurately identifies the pattern and the extent
of the hemangiomatous neovasculature.
- CT scan:
- CT scan of capillary hemangiomas are unrewarding.
- MRI:
- MRI defines the internal characteristics of hemangiomas and clearly
distinguishes it from adjacent muscles.
SURGICAL STAGES:
- In children and adolescents, the majority of hemangiomas are benign,
active stage 2 lesion.
- Occasionally they will permeate through all the tissue barriers in
an aggressive stage 3 fashion.
- Hemangiomas do not undergo malignant transformation.
TREATMENT:
- Intracapsular excision is often followed by recurrence as the
lesion rarely forms a pseudocapsule. It is most often diffusely infiltrative.
- In theory extracapsular excision should provide a definitive procedure
for stage 2 hemangioma, but it is impossible to dissect between the periphery
of the lesion and the normal tissues without inadvertent transsectoin of
occult extensions.
- Wide excision does not always lead to complete cure, and is often injustified
due to excessive morbidity.
- Cryosurgery.
- Injection with sclerosing agents.
DISCUSSION: MANAGEMENT OF SOFT TUMOR OF THE FOOT.
Special attention is required for tumor the foot because:
- The foot is composed of a relative higher concentration of lymphatics
and it also contains numerous tendons passing through synovial sheaths
which lie adjacent to bone and neurovascular structures. Therefore the
distribution of the tumors in the foot is differ from tumors arising elsewhere
in the musculoskeletal system.
- There is little muscular mass to permit adequate surgical margins
of resection in cases of pedal tumors.
- The fascial planes between the rays that leads to the periarticular
soft tissues of the mid-foot have no barrier to proximal or distal extension
and are extra-compartmental. Extension proximally into the leg from lesions
of the foot is uncommon
CLINICAL PRESENTATION:
Lesions about the foot generally present early because:
- The thin soft tissue covering: makes relatively small masses easily
palpable.
- Pain and discomfort is produced by mechanical disruption of the function
of the tightly-bound gliding mechanisms
INCIDENCE:
Kirby (1989) analyzed the cases of 83 patients who had a soft tissue
tumor in the foot. He found that 72 (87%) of the lesions were benign with
ganglion cyst and planter fibromatosis being the most common. Eleven (13%)
were malignant tumors, 5(45%) of which were malignant sarcomas.
Staging Studies:
- X-ray:
- Soft tumors of the foot may present with one or more of the following:
visible soft tissue mass calcification, or secondary osseous involvement.
- CT scan:
- Sections 1.5 -2.0 mm in thickness should be taken through the area
of concern to define the complex anatomy. The small size of the scan with
its lack of resolution and abscence of significant fat planes in the soft
tissue make CT scan of limited value about the foot.
- MRI:
- MRI offers better details of soft tissue tumors and their relationship
to surrounding structures.
- Angiography:
- Angiography is rarely needed unless the surgeon is dealing with a vascular
lesion.
BIOPSY:
Incisions for biopsy are influenced about the foot by the presumptive
clinical diagnosis:
- Lesions that appear benign are best approached with incisions that
match the anatomical creases and that avoid the weight bearing surfaces.
- Malignant lesions should be approached through longitudinal incisions,
bearing in mind the approaches to be used in subsequent wide or radical
local procedures
A marginal excision for diagnosis of a malignant lesion is much
more likely to cause distal extension than is a carefully controlled
incisional biopsy.
SURGICAL STAGES:
- Stage IA, Grade Low, Site Intracompartmental.
- Stage IB, Grade Low, Site Extracompartmental.
- Stage IIA, Grade High, Site Intracompartmental.
- Stage IIB, Grade High, Site Extracompartmental.
- Stage III, Grade Any, Site Any.
SURGICAL LOCATIONS:
- Intracompartmental Intraosseous, Extracompartmental Soft
tissue extension
- Intracompartmental Intra-articular, Extracompartmental
Soft tissue extension
- Intracompartmental Superficial, Extracompartmental Deep
- Intracompartmental Juxtacortical, Extracompartmental
Intraosseous
- Intracompartmental Intrafascial compartments, Extracompartmental
Extrafascial compartments
TREATMENT:
- Stage I and 2 benign lesions are treated by marginal excision.
- Stage 3 benign and stage I malignant soft tissue lesions need wide
excision. In this setting it is rare that a lesion dose not involve the
underlying bone with reactive tissues and frequently lesions extend through
the large vascular perforations into the bone itself. Often an en block
wide excision of skin, subcutaneous tissue, tendons, and parts of various
bones and joints leads to more disability than a partial amputation that
would achieve the same wide margin.
- Stage II soft-tissue lesions in the foot require an amputation to achieve
a radical margin.
REFERENCES:
- Cohen EK, Kressel HY, Preosio T, MR imaging of soft tissue hemangioma:
correlation with pathologic finding. AJR 1988; 150: 1079-1081.
- Enneking WF; Musculoskeletal Tumor Surgery. Churchil, New York, Edinburgh,
London, and Melbourne 1983.
- Enneking WF, Spanier SS, Goodman MA. A system for the surgical staging
of musculoskeletal sarcoma. Clin. Orthop. 1980; 153: 106.
- Keigley BA, Haggar AM, Gaba A, Ellis BI, Froelich JK, Wu KK. Primary
tumors of the foot: MR image. Radiology 1989.
- Kirby EJ, Shereff MJ, Lewis MM. Soft-tumor and tumor-lite lesion of
the foot. An analysis of eighty-three cases. J Bone Joint Surg 1989; 71
(4):621-626.
- Lane JM, Rosenthal HG. Pediatric foot tumors in; The Child's Foot and
Ankle edited by J.C.Drennan, Raven Press, Ltd. New York 1992.
- Seale KS, Lange TA, Manson D, Hackbarth DA. Soft tissue tumor of the
foot and ankle. Foot Ankle 1988; 9(l): 19-27.