SYRINGOMYELIA AND SCOLIOSIS
JEFFREY J. METER, M.D., Orthopaedic Resident
ROBERT STANTON, M.D., Pediatric Orthopaedic Attending
January 16, 1996
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY:
- HISTORY: J.G. is a ten year old female who presented to the Institute
with a spinal curvature noted in a routine camp physical. She had no neurologic
complaints. Her birth, medical, and developmental history were all unremarkable.
Her father has a vague history of spinal curvature.
- PHYSICAL EXAM: Physical examination was significant for a moderate
left thoracic rib prominence as well as absent abdominal reflexes in the
upper and lower quadrants on the left side.
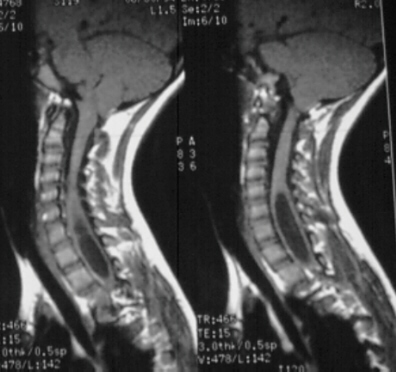
- XRAYS: A 24 degree left thoracic curve from T5 - Tl1
 was noted on scoliosis spine films.With the asymmetric abdominal reflexes
and high thoracic left curve she was sent for an MRI scan. This revealed
a large syringomyelia with dilatation in the lower cervical and upper thoracic
area. Also noted was an Arnold-Chiari malformation.
was noted on scoliosis spine films.With the asymmetric abdominal reflexes
and high thoracic left curve she was sent for an MRI scan. This revealed
a large syringomyelia with dilatation in the lower cervical and upper thoracic
area. Also noted was an Arnold-Chiari malformation. 
- TREATMENT: She was referred to a neurosurgeon who performed a posterior
fossa decompression. She tolerated this well.
- FOLLOW-UP: A year later she had progressed somewhat in her curvature
and bracing was initiated.
Syringomyelia and Scoliosis
Definition of Syringomyelia:
A condition which is defined by a tubular cavity which contains fluid
within the spinal cord.
Types:
- Type I: communicating - connects with posterior fossa.
- Type II: noncommunicating - tumor or traumatic. tense cyst. normal
posterior fossa.
History:
Heavy birthweight, protracted labor, traumatic delivery
Signs and Symptoms:
Symptoms - Headache - worsens with cough, sneeze, strain. Common in
communicating form. Neckache. Body/joint pains - worsens with straining.
Often multiple misdiagnoses - CTS, cubital tunnel... Numbness - may replace
pain
Signs - Horner's syndrome, Nystagmus, Muscle wasting, LE spasticity,
Charcot UE joints, Pes Cavus, Short neck, Low hairline, Limb length inequality,
Hand/foot asymmetry, Diplopia, Giddiness, Dysphagia, Dysphonia, Salivation
Disorder, Sexual dysfunction, Abnormal pain & temperature sensibility,
Asymmetric abdominal reflexes
Radiographic Signs:
Rapidly progressive scoliosis, Upper thoracic curve, Left thoracic curve,
High double thoracic curve, Cervical bony , nomalies, Erosion of cervical
bodies, Widened spinal canal, Basilar invagination, Cervical ribs
Associated with:
Arnold-Chiari malformation, Klippel-Feil, Myelomeningocele
Incidence:
Two American studies quote the incidence of scoliosis in syringomyelia
to be about 60% If a child develops symptoms of scoliosis before age 16
the eventual incidence of scoliosis is 82%, if later than age 16 symptoms
develop, the incidence is 48%.
Diagnosis:
Suspect if C5 canal is 6mm greater than body. If it is 4mm there is
a 3:1 probability of syrinx.
If C5 canal is wider than C6 body - suspect.
Etiology of Scoliosis:
The cystic lesions are typically located dorsal to the central canal.
In this position they are presumed to impinge on the medial nuclear groups
- ventromedial and dorsomedial, and thus affect the anterior horn cells,
thereby affecting the muscles of the trunk in those segments.
Treatment:
Initial treatment involves draining the cyst, observing the spine, and
fusing the spine with progression. Risks of surgery are substantial, with
possible neurologic progression.
References:
- Baker, AS and Dove, J: Progressive Scoliosis as the First Presenting
Sign of Syringomyelia. JBJS, 65-B:472-73. 1983.
- Hubert, HT and MacKinnon, WB: Syringomyelia and Scoliosis. JBJS, 51
B:338-343, 1969.
- Nordwall, A and Wikkelso, C: A Late Neurologic Complication of Scoliosis
Surgery in Connection with Syringomyelia. Acta Orthop Scand, 50:407-410,
1979.
- Weber, FA: The Association of Syringomyelia and Scoliosis. JBJS, 56B:589,1974.
- Williams, B: Orthopaedic Features in the Presentation of Syringomyelia.
JBJS, 61-B:314-323,1979.
- Winter, RB, et al: Prevalence of Spinal Canal or Cord Abnormalities
in Idiopathic, Congenftal, and Neuromuscular Scoliosis. Orthop.Trans.