
MILAN S. MOORE, MD, Resident Orthopaedic Surgery
WILLIAM G. MACKENZIE, MD, Pediatric Orthopaedic Surgery Attending
April 4, 1996
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
While fractures involving the tibia and fibula are the most common lower extremity pediatric fractures, those involving separation of the proximal tibial epiphysis are among the most uncommon but have the highest rate of complication. Neer and Horwitz reported an incidence of 0.8% of 2500 consecutive epiphyseal fractures. Therefore, the general orthopaedist should encounter only a few of these injuries during a lifetime of practice.
A 14 year old Hispanic male presented to an outside institution after sustaining a hyperextension injury to his right knee during a soccer collision. He had the immediate onset of pain and noted swelling of the knee during the first hour after injury. He was unable to bear weight; flexion and extension of the knee exacerbated the pain. He had no previous history of injury to his right lower extremity. Outside records document the following course.
Examination of the right lower extremity was remarkable for a knee effusion with soft tissue swelling and diffuse tenderness at the proximal tibia. The patient was unable to dorsiflex or evert his foot. Sensation along the lateral calf and foot was diminished. The dorsalis pedis and tibialis anterior pulses were palpable and there was good distal capillary refill.
AP and lateral views of the right lower extremity revealed a Salter
Harris III proximal tibial fracture with intraarticular extension into
the medial and lateral tibial plateaus. The epiphysis was anteriorly displaced
on the metaphysis.
The patient underwent closed reduction and application of a long leg splint on the night of injury. Notes document a palpable dorsalis pedis pulse after reduction. The patient presented again in the ER two days after injury with complaints of weakness of toe movement and forefoot pain. The splint was loosened.
He was seen in orthopaedic follow up two days later at which time he was found to have diffuse swelling from the mid thigh distally, diminished sensation of the lateral foot, cyanosis of the dorsum of the foot, fever to 101.5, and poorly dopplerable pulses at the popliteal, posterior tibial, and dorsalis pedis arteries. He underwent a venous duplex ultrasound of the right lower extremity without findings of deep venous thrombosis.
He was taken to surgery where fasciotomies of the right leg were performed. Exploration of the popliteal artery at the level of the fracture revealed it to be contused and occluded. A reverse saphenous vein bypass graft was placed and angiogram revealed flow into the posterior tibial artery. The postoperative course was complicated by myoglobinuria, anterior tibial and dorsalis pedis occlusion, muscle necrosis treated by sequential debridement, and wound infection with methacillin resistant Staph. epidermidis.
Seventeen days after the original injury the forefoot was frankly gangrenous
and an open transmetatarsal amputation was performed  .
Anterior and lateral compartment debridement of non-viable muscle left
the fibula exposed, and it was resected. The lateral tibia was drilled.
The patient underwent repeat debridements and whirlpool therapy with his
clinical course complicated by Pseudomonal infection of the wounds. He
underwent closure of his transmetatarsal amputation and split thickness
skin graft to his lateral wounds 88 days after injury.
.
Anterior and lateral compartment debridement of non-viable muscle left
the fibula exposed, and it was resected. The lateral tibia was drilled.
The patient underwent repeat debridements and whirlpool therapy with his
clinical course complicated by Pseudomonal infection of the wounds. He
underwent closure of his transmetatarsal amputation and split thickness
skin graft to his lateral wounds 88 days after injury.
The patient presented to A.I. DuPont 15 days later (103 days after injury)
with serosanguinous drainage from the upper portion of his lateral wound.
Irregular areas of sclerosis and lucency of the tibia on plain films and
CT 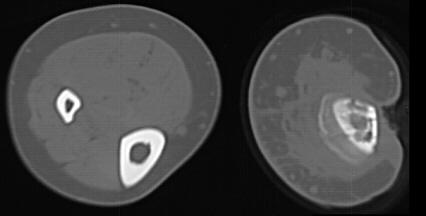 as well as irregular uptake on bone scan
as well as irregular uptake on bone scan  suggested areas of necrotic bone and chronic osteomyelitis. A hand film
showed a bone age of 17 and scanogram documented a 2 cm leg length discrepancy.
A lateral cortical tibial sequestrum gradually demarcated. He was followed
for a year without lasting resolution of his drainage and underwent sequestrectomy
and open packing of the wound.
suggested areas of necrotic bone and chronic osteomyelitis. A hand film
showed a bone age of 17 and scanogram documented a 2 cm leg length discrepancy.
A lateral cortical tibial sequestrum gradually demarcated. He was followed
for a year without lasting resolution of his drainage and underwent sequestrectomy
and open packing of the wound.
Now two years after injury, he remains on oral antibiotics; the lateral wound has gradually closed and is without drainage. He has a 2 cm leg length discrepancy and no angulatory deformity. Knee range of motion is 0 to 110 degrees and there is no ligamentous instability. He is an independent ambulator in a boot with spacer and denies knee or leg pain.
Proximal Epiphysis is relatively well protected from deforming forces
Yet when displacement occurs, the popliteal artery is vulnerable
Salter-Harris Classification |
Aitken |
Burkhart Peterson |
Shelton Canale |
Total |
I |
- |
3 |
9 |
12 (15%) |
II |
9 |
9 |
17 |
35 (43%) |
III |
2 |
6 |
10 |
18 (22%) |
IV |
3 |
8 |
3 |
14 (27%) |
V |
- |
2 |
- |
2 (3%) |
Total |
- | - | - |
81 |
SH I Half are non-displaced and diagnosed by stress radiographs. Earlier age (average 10 yrs of age)
SH II Most common type. One-third are non-displaced
SH III Often associated with lateral condyle fractures or MCL injury
SH IV Often with angular deformity
SH V Retrospective diagnosis. Anterior physeal closure can cause significant genu recurvatum
DIRECT
INDIRECT
Tenderness over proximal tibial growth plate 1-1.5 cm distal to joint line
Anterior concavity in displaced fractures
Oblique and stress radiographs useful
Evaluation much include careful neurovascular exam.
Assess popliteal artery integrity with any significant displacement, especially in hyperextension injuries.
NON - DISPLACED |
ALL |
Long leg bivalved cast with 30% knee flexion |
DISPLACED |
SH II |
Closed reduction, bent knee cast. ORIF if cannot get or maintain reduction |
| - |
SH III or SH IV |
Closed reduction and percutaneous pinning or Open reduction and pinning |
VASCULAR INSUFFICIENCY
PERONEAL NERVE PALSY
DISPLACEMENT OF CASTED FRACTURES
PREMATURE GROWTH ARREST