TORTICOLLIS CAUSED BY INTERVERTEBRAL DISC CALCIFICATION
TOBENNA OKEZIE, M.D., Orthopaedic Surgery Resident
S. JAY KUMAR M.D., Attending Pediatric Orthopaedic Surgeon
February 21, 1996
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY
Patient is a 4 year old male who developed the insidious onset of neck
pain and stiffness 4 days prior to admission. Over the intervening period,
the patient suffered from worsening of his symptoms which led to increasing
irritability and difficulty sleeping. On the day of admission, he was seen
by a local pediatrician for severe neck pain. It was observed that his
head was in a fixed position just slightly right of midline. The patient's
past medical history was remarkable for two recent self-limited episodes
of hives and urticaria on his trunk and extremities that was treated with
prednisone. There was vague history of remote trauma about one month previously
when the patient had been "horsing" around with his brother.
The child had no evidence of a viral prodrome, constitutional symptoms
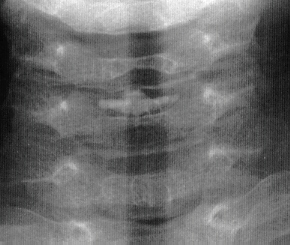
or travel history. He was sent to a local hospital where radiographs of
the cervical spine demonstrated calcifications in the C3-4 and C5-6 intervertebral
disc spaces
 .
Neurological exam was normal. The child's pain was refractory to morphine
treatment and he was transferred to A.I. for the management of his intractable
pain. On arrival, his physical exam was unchanged. Blood work revealed
a WBC count of 12.7K with 75% PMNs and an ESR of 80. Radiographs of spine
showed the presence of an addition calcification in his thoracic spine
.
Neurological exam was normal. The child's pain was refractory to morphine
treatment and he was transferred to A.I. for the management of his intractable
pain. On arrival, his physical exam was unchanged. Blood work revealed
a WBC count of 12.7K with 75% PMNs and an ESR of 80. Radiographs of spine
showed the presence of an addition calcification in his thoracic spine

 .
He was treated with oral valium and a soft cervical collar. Over the ensuing
24 hrs the child demonstrated marked improvement of his symptoms and was
switched to motrin. He was subsequently discharged.
.
He was treated with oral valium and a soft cervical collar. Over the ensuing
24 hrs the child demonstrated marked improvement of his symptoms and was
switched to motrin. He was subsequently discharged.
TORTICOLLIS CAUSED BY INTERVERTEBRAL DISC CALCIFICATION
Calcification of intervertebral discs is not uncommon in adults and
is usually considered a sign of degeneration due to normal aging without
specific clinical or anatomic significance.
Pediatric disc calcification was first described by Baron in 1924 and
since that time more than 100 cases have been reported. It is slightly
more common in boys than girls (7:5 ratio) with an average age of presentation
of 8 years (range 8 days to 13 years)
It is most common in the cervical spine, where it is especially symptomatic.
Asymptomatic lesions have been detected in the thoracic spine on routine
chest radiographs.
ETIOLOGY
This is unclear. Recognized causes of calcification in adult intervertebral
disc such as hyperparathyroidism, hemochromatosis and ochronosis have not
been implicated in children.
In addition, other causes of calcification in pediatric connective tissues,
including hypervitaminosis D and chrondrocalcinosis, have not been found
to be associated with calcification of intervertebral discs. There is no
evidence available to suggest that a metabolic defect is present.
Pathophysiology appears to involve calcification of the nucleus pulposus.
The annular ligament is spared. The calcified nucleus pulposus may herniate
anteriorly into the prevertebral soft tissues or posteriorly into the spinal
canal. Changes have been observed in vertebral bodies, but there clinical
significance is unclear.
There is a history of antecedent trauma in only about (30%) and upper
respiratory infection in (15% with a latent period between 5 days and 3
week.
SIGNS AND SYMPTOMS
Onset of symptoms is abrupt, usually between 12 and 48 hours. Common
symptoms are neck pain, spasm torticollis and reduced range of motion.
Infrequently, dysphagia or long tract signs will be observed.
Fever has been observed in 23% of patients. A significant elevation
of white cell count has rarely been observed
XRAYS
The number of calcified discs varied from 1 to 12 (mean 1.69) . Symptomatic
calcified discs are most common at C6-7. Radiologic examination shows images
of calcium density in the normally radiolucent intervertebral discs. Anterior
or posterior protrusion can be observed. The lesions demonstrate high density
on CT and low signal intensity on MRI.
TREATMENT
The natural history is typically one of complete clinical radiographic
resolution. Two-thirds of patients are free of symptoms within 3 weeks
and 95% within 6 months. The radiographs show regression or disappearance
of the calcified deposits in 90%. In the absence of compression of the
spinal cord conservative management is preferred. The use sedatives analgesics
and cervical traction are tailored to the symptoms. The use of a soft cervical
collar and avoidance of body contact sports may be prudent.
One case has been reported in which an anterior cervical discectomy
was performed after six weeks of unsuccessful conservative management in
al child with a severe radiculopathy.
REFERENCES
- Caffey, J.: Pediatric X-ray diagnosis
- Herring J.A. Cervical disc calcification: Instructional Case Journal
of Pediatric Orthopaedics vol 8: 613-616 1988
- Loder, R., Hensinger, R.N., Developmental Abnormalities of the Cervical
Spine Chapter 17 In The Pediatric spine :Principles and Practice , S.L.
Weinstein, Editor Raven Press Ltd., New York 1994
- Sonnabend, D.H., Taylor, T.K.F., Chapman, G.K. : Intervertebral disc
calcification syndromes in Children JBJS 64-B p.25-31
 .
Neurological exam was normal. The child's pain was refractory to morphine
treatment and he was transferred to A.I. for the management of his intractable
pain. On arrival, his physical exam was unchanged. Blood work revealed
a WBC count of 12.7K with 75% PMNs and an ESR of 80. Radiographs of spine
showed the presence of an addition calcification in his thoracic spine
.
Neurological exam was normal. The child's pain was refractory to morphine
treatment and he was transferred to A.I. for the management of his intractable
pain. On arrival, his physical exam was unchanged. Blood work revealed
a WBC count of 12.7K with 75% PMNs and an ESR of 80. Radiographs of spine
showed the presence of an addition calcification in his thoracic spine