CONGENITAL RADIOULNAR SYNOSTOSIS
STEVEN R. BOYEA, M.D., Resident, Orthopaedic Surgery
WILLIAM MACKENZIE, M.D., Attending, Pediatric Orthopaedic Surgery
20 March 1996
CLINICAL CASE PRESENTATION
ORTHOPAEDIC DEPARTMENT
THE ALFRED I. DUPONT INSTITUTE
WILMINGTON, DELAWARE
CASE HISTORY:
The patient is a 11 year old who presented for evaluation of his left
arm. He states he has always had limited range of motion of his left arm,
however, his mother states that it was not until recently she became concerned.
The patient is right hand dominant. He denies any weakness or loss of feeling
in his left hand or arm. He states that some movements are more difficult
than others especially around the elbow. The child has no significant past
medical history and has had a normal developmental history except for the
left arm. He denies any trauma to the elbow or fractures/dislocations.
This does not cause him any functional problems and he has no pain.
PHYSICAL EXAM:
The left arm demonstrates a shoulder with FROM and strength 5/5. The
elbow has a flexion from 0 to 135 degrees, but the forearm is fixed in
45 degrees of pronation without active or passive supination. The wrist
has FROM with some hypermobility, especially in radial and ulnar deviation.
The strength is 5/5 in elbow flexion/extension, wrist flexion/extension
and grip. He is neurovascularly, intact. The right arm also demonstrates
normal motion at the elbow with flexion from 0-135 degrees but limited
supination from 0-50 degrees and pronation from 0-20 degrees. The remainder
of his exam was normal.
RADIOGRAPHS:
These demonstrate the left elbow to have a bony synostosis of the proximal
radius and ulna, distal to the proximal radial physis but with anterior
dislocation of the radial head. There is no evidence of a bony synostosis
or dislocation in the right elbow. Internal Rotation  ,
External Rotation
,
External Rotation  ,
AP
,
AP  ,
Lateral
,
Lateral  .
.
ASSESSMENT:
- Left proximal radioulnar osseous synostosis
- Right proximal radioulnar fibrous synostosis
TREATMENT:
CONGENITAL RADIOULNAR SYNOSTOSIS
Embryology
- anomaly of longitudinal segmentation
- upper limb bud arises at 26 days of age
- growth and differentiation continue until 46 days of age
- at 35 days the elbow is 3 connected cartilaginous anlage
- longitudinal segmentation produces separation of the distal radius
and ulna
- for a time the proximal radius and ulna are united and share a common
perichondrium
- abnormal genetic or teratogenic factors operating at this time would
interfere with proximal radioulnar joint morphogenesis
Epidemiology
- usually sporadic, can be associated with family history, autosomal
dominant with variable expression
- 60% bilateral
- equal male to female distribution
- associated skeletal anomalies
- DDH
- club feet
- missing or diminutive thumb
- coalescence of carpal bones
- symphalangism
- dislocation of radius
- associated syndromes
- Aperts
- Williams
- Klinefelter's
- Nievergelt-Pearlman
- acrocephalopolysyndactyly
Clinical Features
- average age abnormality observed 2.5 yo
- functional complaints
- difficulty holding or using small objects
- inability to dress themselves
- backhanded position in holding objects
- difficulty feeding themselves
- inability to accept small objects in their hands
- difficulty competing in sports involving upper extremities
- decreased carrying angle
- average fixed flexion contracture was 16 degrees
- forearm shortening
- hypermobility of wrist
- fixed pronation ranges from 15 to 150 degrees
Radiographic Features
- spectrum of anatomic variation
- range of synostosis from proximal fibrous union to total synostosis
of radius and ulna
- absence of/or radial head deformity
- radial head dislocation
- forearm shortening
- varying continuity of cancellous bone throughout the coalition
- radial shaft bowing
Classification
- Original
- Type 1: proximal or true radioulnar synostosis in were the radius and
ulna are smoothly fused at their proximal borders for a variable distance.
- Type 2: radioulnar synostosis with congenital dislocation of the head
of the radius in which the fusion is just distal to the proximal radial
epiphysis.
- Modified (Cleary et al., "Congenital Proximal Radio-Ulnar Synostosis."
JBJS, 67-A:4, 1985.)
- Type I: synostosis does not involve bone, associated with reduced radial
head.
- Type II: visible osseous synostosis, associated with normal reduced
radial head.
- Type III: visible osseous synostosis with a hypoplastic and posteriorly
dislocated radial head.
- Type IV: short osseous synostosis with an anteriorly dislocated mushroom
shaped radial head.
Management
Observation
- NO functional deficits
- fixed pronation of 15 degrees or less
Surgical correction
- functional loss of forearm axial rotation
- fixed pronation of greater than 60 degrees (particularly with bilateral
deformities)
Methods
Taking down the synostosis and interposition of soft tissue
- poor results
- narrowing of interosseous membrane
- loss of correction with refusion
Kelikian/Doumanian swivel
- resection of a piece of proximal radius and insertion of swivel.
- simultaneous transfer of FCR, FCU or EDU for active supination
- failure secondary to loosening of swivel, swivel failure
Derotational osteotomy distal to synostosis site
- rotation of forearm to improved position distal to osteotomy
- fixation was with K-wires, Steinman pins or staples
- failure from loss of rotation secondary to tight interosseous membrane
- significant risk of vascular compromise secondary to functional shortening
of arteries of forearm
- the further the osteotomy from the synostosis the greater the vascular
risk
Derotational osteotomy through the synostosis mass
- osteotomy through the synostosis with rotation to more functional position
- position held with pins, external fixator or plaster until synostosis
reforms
- usual loss of 15 degrees of original correction
- Simmons et al. in 1983, Kahalil and Vizkelety in 1993 demonstrated
good functional out comes
- bilateral cases should have one hand in slight pronation and the other
in neutral position
Derotational osteotomy with the Ilizarov Method
- osteotomy through the synostosis
- fixation proximally with hybrid fixation
- fixation distally with half pins
- Ilizarov device with rotation/translation hinges
- rotation at a rate of 4 degrees per day
- low risk of vascular injury because of slow rotational correction
- REFERENCES:
- Bolano, L.E. Congenital Proximal Radioulnar Synostosis: Treatment with
the Ilizarov Method. J Hand Surg 19A: 977-978, 1994.
- Charvat, K.A.; Hornstein, L.; Oestreich, A.E. Radio-ulnar synostosis
in Williams syndrome: A frequently associated anomaly. Pediatr Radiol 21:
508-510, 1991.
- Cleary, J.E.; Omer, G.E., Jr. Congenital proximal radio-ulnar synostosis:
Natural history and functional assessment. J Bone Joint Surg 67-A: 539-545,
1985.
- Kelikain, H.; Doumanian, A. Swivel for proximal radio-ulnar synostosis.
J Bone Joint Surg 39-A: 945-952, 1957.
- Khalil, I.; Vizkelety, T. Osteotomy of the synostosis mass for the
treatment of congenital radio-ulnar synostosis. Arch Orthop Trauma Surg
113: 20-22, 1991.
- Mital, M.A. Congenital radioulnar synostosis and congenital dislocation
of the radial head. Orthop Cln N Am 7: 375-383, 1976.
- Simmons, B.P.; Southmayd, W.W.; Riseborough, E.J. Congenital radioulnar
synostosis. J Hand Surg 8: 829-838, 1983.
- Wiley, J.J.; Loehr, J.; McIntyre, W. Isolated dislocation of the radial
head. Orthop Rev 20: 973-976, 1991.
[Orthopaedic Department Home Page,
Resident Education Home Page, Back
to Question Module, Back to Case Presentations,
Top(Congenital Radioulnar Synostosis).
 ,
External Rotation
,
External Rotation 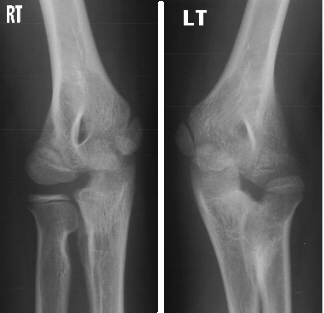 ,
AP
,
AP  ,
Lateral
,
Lateral 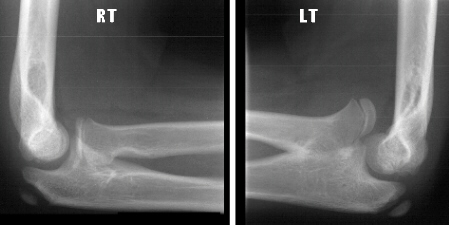 .
.